

The societal economic burden of autosomal dominant polycystic kidney disease in the United States
- PMID: 32070341
- PMCID: PMC7029467
- DOI: 10.1186/s12913-020-4974-4
The societal economic burden of autosomal dominant polycystic kidney disease in the United States
Abstract
Background: Autosomal dominant polycystic kidney disease (ADPKD) is one of the most common inherited kidney diseases characterized by progressive development of renal cysts and numerous extra-renal manifestations, eventually leading to kidney failure. Given its chronic and progressive nature, ADPKD is expected to carry a substantial economic burden over the course of the disease. However, there is a paucity of evidence on the impact of ADPKD from a societal perspective. This study aimed to estimate the direct and indirect costs associated with ADPKD in the United States (US).
Methods: A prevalence-based approach using data from scientific literature, and governmental and non-governmental organizations was employed to estimate direct healthcare costs (i.e., medical services, prescription drugs), direct non-healthcare costs (i.e., research and advocacy, donors/recipients matching for kidney transplants, transportation to/from dialysis centers), and indirect costs (i.e., patient productivity loss from unemployment, reduced work productivity, and premature mortality, caregivers' productivity loss and healthcare costs). The incremental costs associated with ADPKD were calculated as the difference between costs incurred over a one-year period by individuals with ADPKD and the US population. Sensitivity analyses using different sources and assumptions were performed to assess robustness of estimates and account for variability in published estimates.
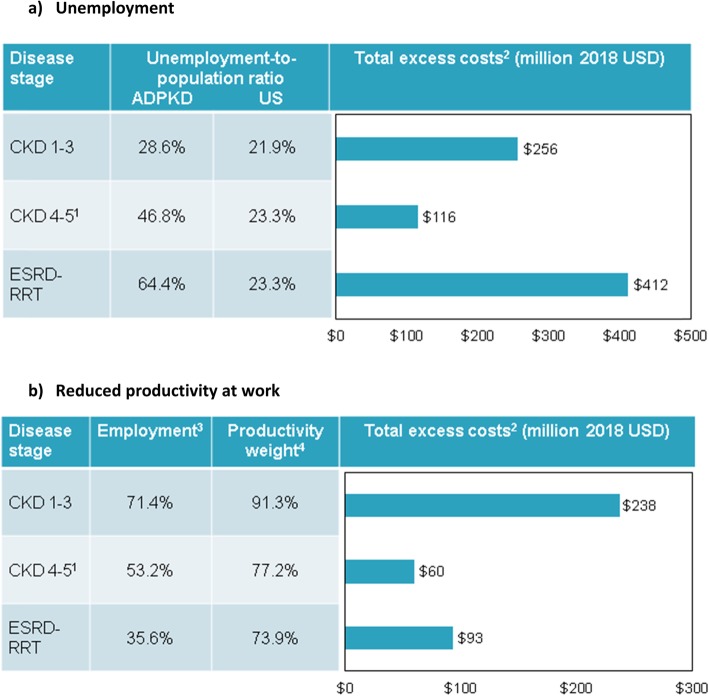
Results: The estimated total annual costs attributed to ADPKD in 2018 ranged from $7.3 to $9.6 billion in sensitivity analyses, equivalent to $51,970 to $68,091 per individual with ADPKD. In the base scenario, direct healthcare costs accounted for $5.7 billion (78.6%) of the total $7.3 billion costs, mostly driven by patients requiring renal replacement therapy ($3.2 billion; 43.3%). Indirect costs accounted for $1.4 billion (19.7%), mostly driven by productivity loss due to unemployment ($784 million; 10.7%) and reduced productivity at work ($390 million; 5.3%). Total excess direct non-healthcare costs were estimated at $125 million (1.7%).
Conclusions: ADPKD carries a considerable economic burden, predominantly attributed to direct healthcare costs, the majority of which are incurred by public and private healthcare payers. Effective and timely interventions to slow down the progression of ADPKD could substantially reduce the economic burden of ADPKD.
Keywords: Autosomal dominant polycystic kidney disease; Burden of disease; Direct costs; Indirect costs; Societal impact.
Conflict of interest statement
MC, AMM, AG, and MGL are employees of Analysis Group, Inc., that has received consultancy fees from Otsuka Pharmaceutical Development & Commercialization, Inc. MSA and DO are employees of Otsuka Pharmaceutical Development & Commercialization, Inc., and may own stocks/stock options.
Figures


References
-
- National Institutes of Health . Fact Sheet: Autosomal Dominant Polycystic Kidney Disease. 2010.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
