

Biceps tenotomy versus tenodesis: patient-reported outcomes and satisfaction
- PMID: 32070381
- PMCID: PMC7029563
- DOI: 10.1186/s13018-020-1581-3
Biceps tenotomy versus tenodesis: patient-reported outcomes and satisfaction
Abstract
Background: Biceps tenotomy and tenodesis are surgical treatments for pathology of the proximal tendon of the long head of the biceps. There is debate over which procedure provides better patient outcomes.
Purpose: Compare patient-reported outcomes and satisfaction between biceps tenotomy and tenodesis.
Methods: This retrospective cohort study including all patients undergoing arthroscopic biceps tenodesis or tenotomy as part of more extensive shoulder surgery with a single surgeon. Concomitant procedures included rotator cuff repair, subacromial decompression, acromioclavicular joint resection, and debridement. Patients 36-81 years old were contacted by phone at > 2-year post-operatively to complete a biceps-specific outcome questionnaire. Subject decision not to participate was the sole exclusion criterion. Satisfaction scores and frequencies of potential biceps-related downsides (biceps cramping/spasms, biceps pain, shoulder pain, weakness, cosmetic deformity) were analyzed for the effects of procedure, sex, and age.
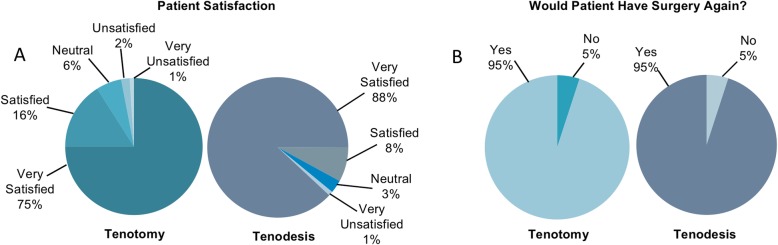
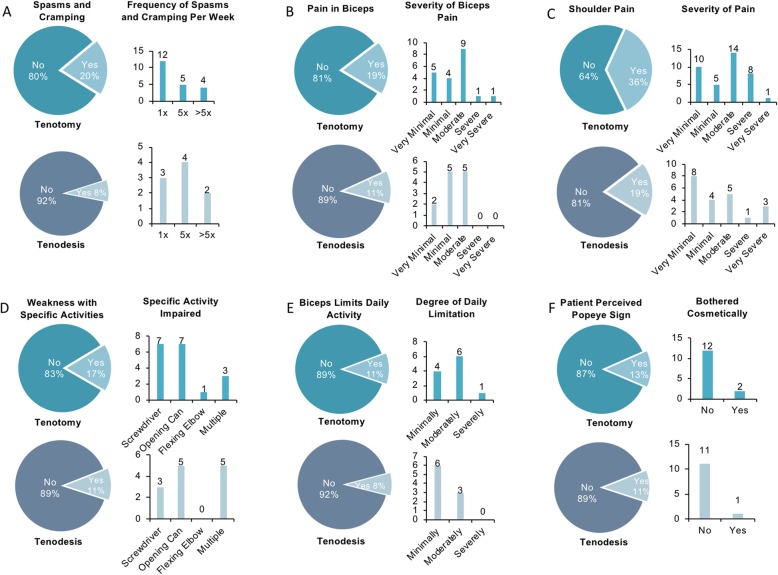
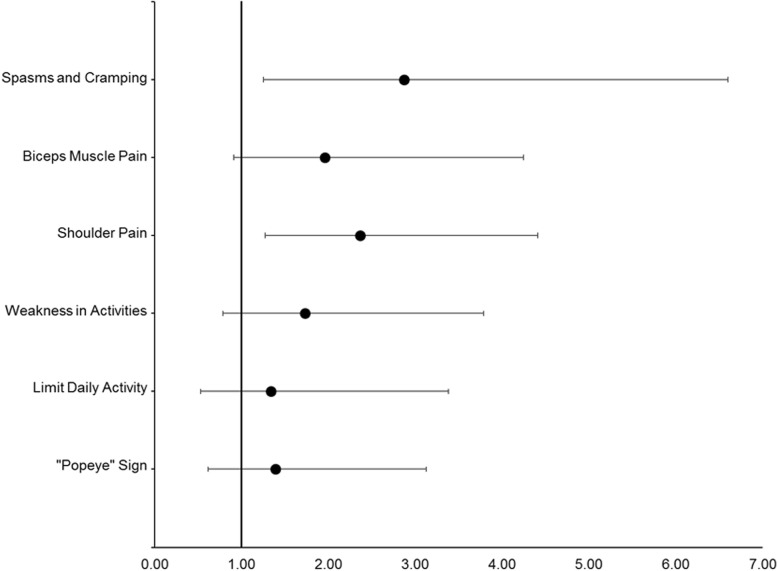
Results: Satisfaction score distributions were similar between patients with tenodesis and patients with tenotomy (χ2 = 8.34, P = 0.08), although slightly more patients with tenodesis than patients with tenotomy reported being satisfied or very satisfied (96% versus 91%). Perceived downsides occurred more frequently among patients with tenotomy than in patients with tenodesis: 59% of patients with tenotomy reported ≥ 1 downside, versus 37% of patients with tenodesis (P < 0.01). In patients reporting ≥ 1 downside, distributions of total downsides differed between procedures (χ2 = 10.04, P = 0.04): patients with tenotomy were more likely to report multiple concurrent downsides than were patients with tenodesis (31% versus 16%). Each individual downside tended to be reported as present by a greater proportion of patients with tenotomy than patients with tenodesis. Sex had no effect on satisfaction or downsides, but there was a trend for older patients to report higher satisfaction and fewer downsides.
Conclusions: Biceps tenotomy and tenodesis are both viable treatments for proximal biceps tendon pathology, yielding high patient satisfaction. There were trends toward greater satisfaction and fewer problems in patients with tenodesis. Still, younger patients with tenodesis did report perceived downsides. Alternatively, older patients tended to be more satisfied with both procedures overall. Regardless of procedure, most patients receiving either tenotomy or tenodesis would undergo their respective surgery again.
Level of evidence: Level III evidence, retrospective comparative cohort study.
Keywords: Biceps tendon; Downsides; Shoulder arthroscopy; Shoulder pain; Spasms/cramping.
Conflict of interest statement
JOA reports no competing interests. BDM reports no competing interests. AWF reports no competing interests. KFB reports the following competing interests: Royalties from Zimmer Biomet Holdings, LLC. Consulting for Abryx, Smith and Nephew, DePuy Orthopaedics, and Pacira Pharmaceuticals Inc. Education for Arthrex Inc., and Supreme Orthopedic Systems, LLC. KFB is also currently working on a new biceps tenodesis device with Smith and Nephew Inc. Further information regarding competing interests can be provided on request.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
