

Defining persistent critical illness based on growth trajectories in patients with sepsis
- PMID: 32070393
- PMCID: PMC7029548
- DOI: 10.1186/s13054-020-2768-z
Defining persistent critical illness based on growth trajectories in patients with sepsis
Abstract
Background: Persistent critical illness is common in critically ill patients and is associated with vast medical resource use and poor clinical outcomes. This study aimed to define when patients with sepsis would be stabilized and transitioned to persistent critical illness, and whether such transition time varies between latent classes of patients.
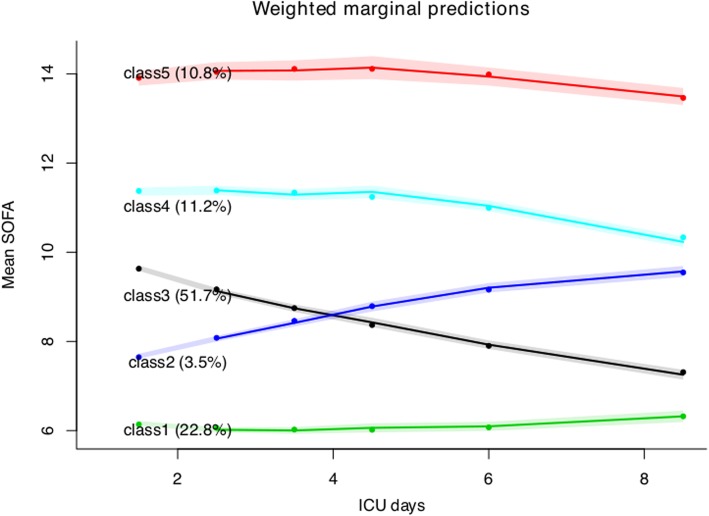
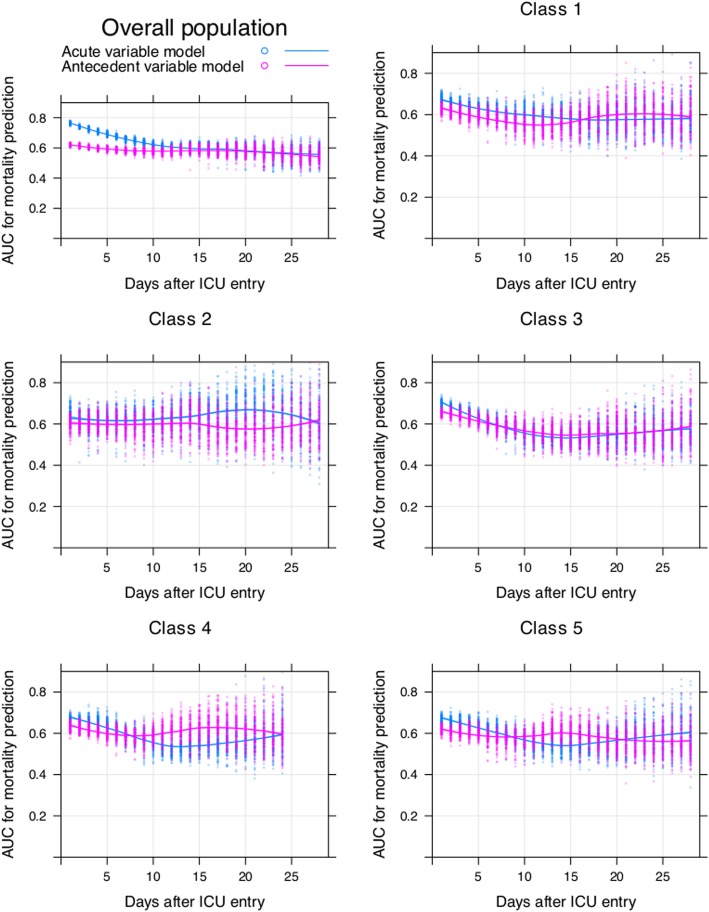
Methods: This was a retrospective cohort study involving sepsis patients in the eICU Collaborative Research Database. Persistent critical illness was defined at the time when acute physiological characteristics were no longer more predictive of in-hospital mortality (i.e., vital status at hospital discharge) than antecedent characteristics. Latent growth mixture modeling was used to identify distinct trajectory classes by using Sequential Organ Failure Assessment score measured during intensive care unit stay as the outcome, and persistent critical illness transition time was explored in each latent class.
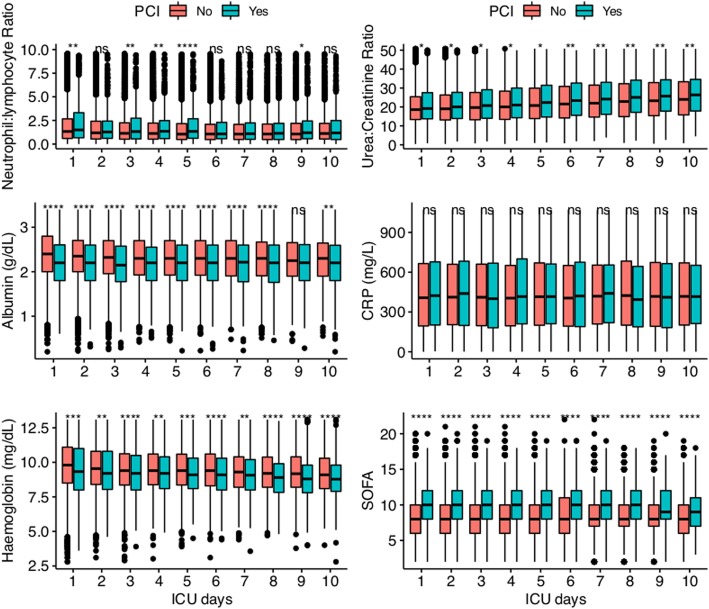
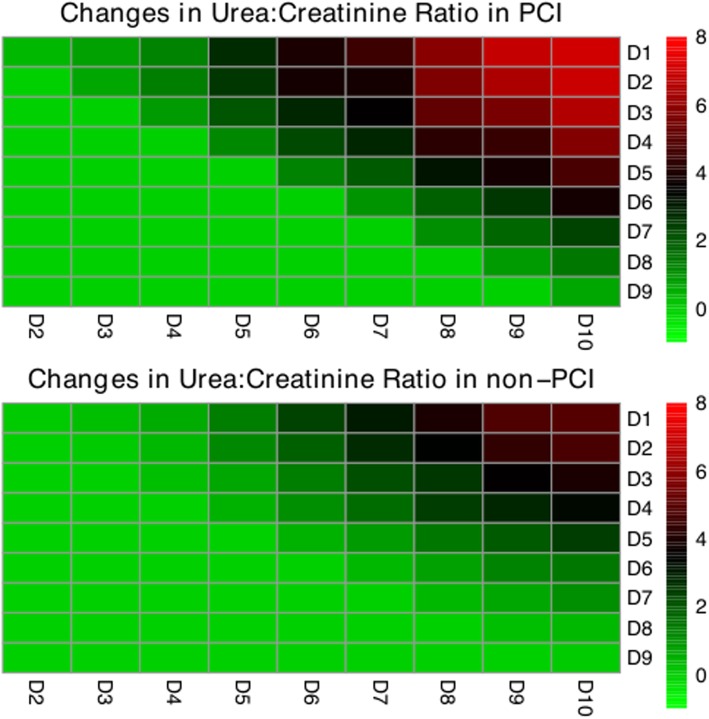
Results: The mortality was 16.7% (3828/22,868) in the study cohort. Acute physiological model was no longer more predictive of in-hospital mortality than antecedent characteristics at 15 days after intensive care unit admission in the overall population. Only a minority of the study subjects (n = 643, 2.8%) developed persistent critical illness, but they accounted for 19% (15,834/83,125) and 10% (19,975/198,833) of the total intensive care unit and hospital bed-days, respectively. Five latent classes were identified. Classes 1 and 2 showed increasing Sequential Organ Failure Assessment score over time and transition to persistent critical illness occurred at 16 and 27 days, respectively. The remaining classes showed a steady decline in Sequential Organ Failure Assessment scores and the transition to persistent critical illness occurred between 6 and 8 days. Elevated urea-to-creatinine ratio was a good biochemical signature of persistent critical illness.
Conclusions: While persistent critical illness occurred in a minority of patients with sepsis, it consumed vast medical resources. The transition time differs substantially across latent classes, indicating that the allocation of medical resources should be tailored to different classes of patients.
Keywords: Persistent critical illness; Sepsis; Unsupervised machine learning.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Iwashyna TJ, Hodgson CL, Pilcher D, Bailey M, van Lint A, Chavan S, et al. Timing of onset and burden of persistent critical illness in Australia and New Zealand: a retrospective, population-based, observational study. Lancet Respir Med. 2016;4:566–573. doi: 10.1016/S2213-2600(16)30098-4. - DOI - PubMed
-
- Bagshaw SM, Stelfox HT, Iwashyna TJ, Bellomo R, Zuege D, Wang X. Timing of onset of persistent critical illness: a multi-centre retrospective cohort studySpringer. Intensive Care Med. 2018;182:446–411. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
