

Driving Pressure During General Anesthesia for Open Abdominal Surgery (DESIGNATION): study protocol of a randomized clinical trial
- PMID: 32070400
- PMCID: PMC7029544
- DOI: 10.1186/s13063-020-4075-z
Driving Pressure During General Anesthesia for Open Abdominal Surgery (DESIGNATION): study protocol of a randomized clinical trial
Abstract
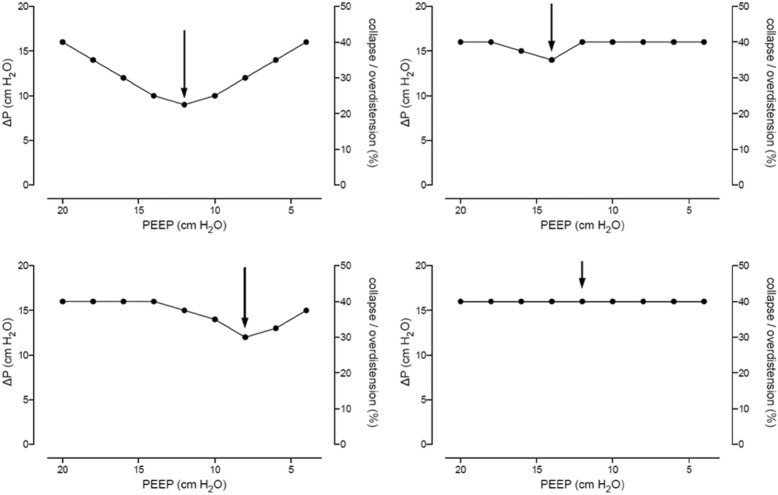
Background: Intraoperative driving pressure (ΔP) is associated with development of postoperative pulmonary complications (PPC). When tidal volume (VT) is kept constant, ΔP may change according to positive end-expiratory pressure (PEEP)-induced changes in lung aeration. ΔP may decrease if PEEP leads to a recruitment of collapsed lung tissue but will increase if PEEP mainly causes pulmonary overdistension. This study tests the hypothesis that individualized high PEEP, when compared to fixed low PEEP, protects against PPC in patients undergoing open abdominal surgery.
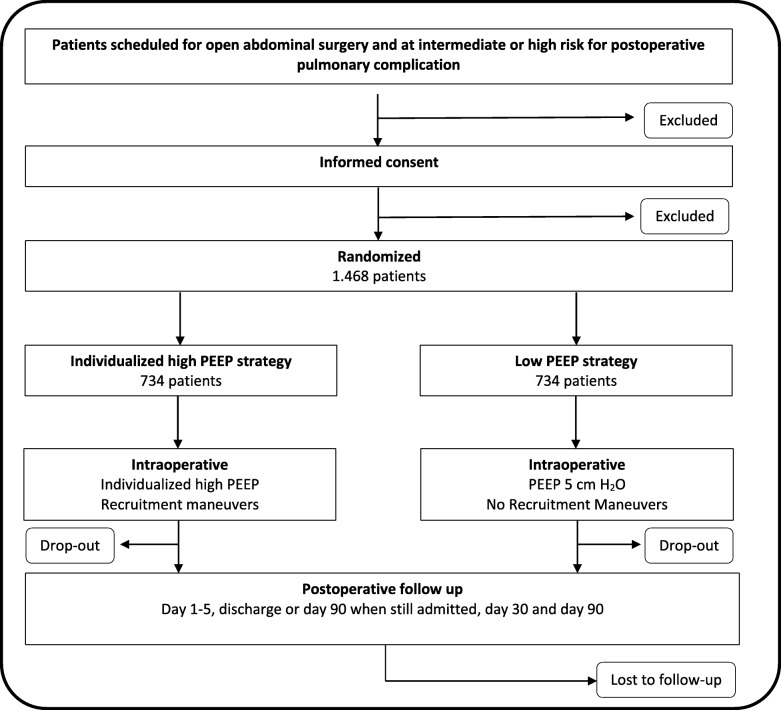
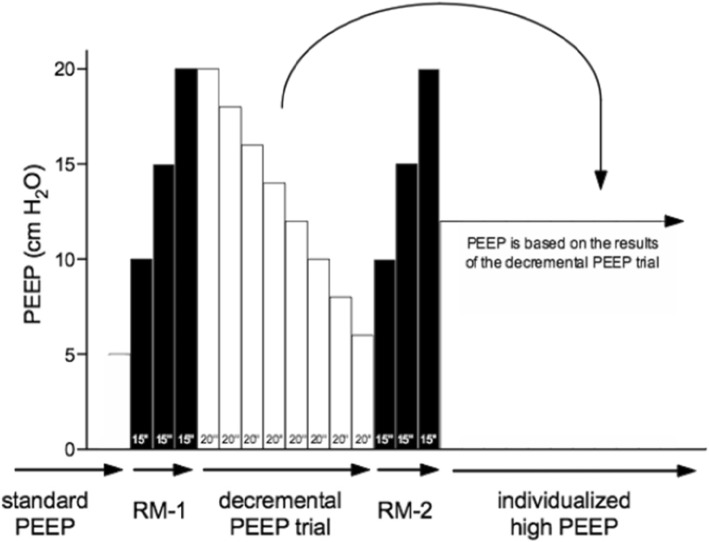
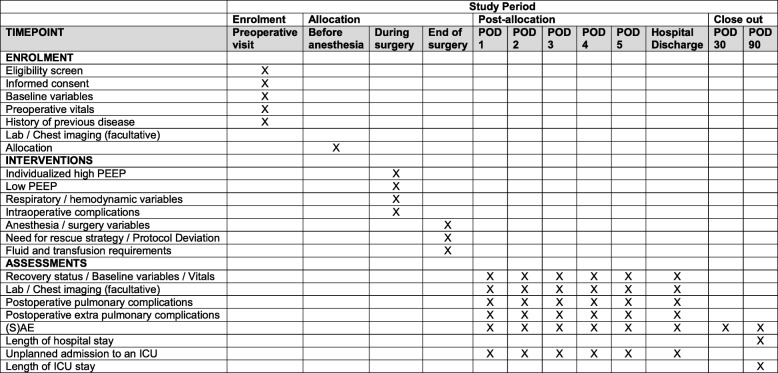
Methods: The "Driving prESsure durIng GeNeral AnesThesIa for Open abdomiNal surgery trial" (DESIGNATION) is an international, multicenter, two-group, double-blind randomized clinical superiority trial. A total of 1468 patients will be randomly assigned to one of the two intraoperative ventilation strategies. Investigators screen patients aged ≥ 18 years and with a body mass index ≤ 40 kg/m2, scheduled for open abdominal surgery and at risk for PPC. Patients either receive an intraoperative ventilation strategy with individualized high PEEP with recruitment maneuvers (RM) ("individualized high PEEP") or one in which PEEP of 5 cm H2O without RM is used ("low PEEP"). In the "individualized high PEEP" group, PEEP is set at the level at which ΔP is lowest. In both groups of the trial, VT is kept at 8 mL/kg predicted body weight. The primary endpoint is the occurrence of PPC, recorded as a collapsed composite of adverse pulmonary events.
Discussion: DESIGNATION will be the first randomized clinical trial that is adequately powered to compare the effects of individualized high PEEP with RM versus fixed low PEEP without RM on the occurrence of PPC after open abdominal surgery. The results of DESIGNATION will support anesthesiologists in their decisions regarding PEEP settings during open abdominal surgery.
Trial registration: Clinicaltrials.gov, NCT03884543. Registered on 21 March 2019.
Keywords: Compliance; Intraoperative ventilation; Mechanical ventilation; Positive end-expiratory pressure; Postoperative complications; Postoperative pulmonary complications; Pulmonary complications; Recruitment maneuver; ΔP.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Serpa Neto A, Hemmes SN, Barbas CS, Beiderlinden M, Fernandez-Bustamante A, Futier E, et al. Incidence of mortality and morbidity related to postoperative lung injury in patients who have undergone abdominal or thoracic surgery: a systematic review and meta-analysis. Lancet Respir Med. 2014;2(12):1007–1015. doi: 10.1016/S2213-2600(14)70228-0. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
