

Effect of salt reduction interventions in lowering blood pressure in Chinese populations: a systematic review and meta-analysis of randomised controlled trials
- PMID: 32071177
- PMCID: PMC7044858
- DOI: 10.1136/bmjopen-2019-032941
Effect of salt reduction interventions in lowering blood pressure in Chinese populations: a systematic review and meta-analysis of randomised controlled trials
Abstract
Rationale and objective: Salt reduction remains a global challenge and different salt reduction strategies have been studied in China. This study is to systematically evaluate evidence from randomised controlled trials (RCT) in China and inform the effective salt reduction strategies.
Design: Systematic review and meta-analysis.
Data sources: MEDLINE, Embase, Cochrane Central Register of Controlled Trials, Wanfang Data and the China National Knowledge Infrastructure databases through October 2019.
Eligibility criteria: RCTs conducted in China with at least 4 weeks' duration of study and blood pressure (BP) reported.
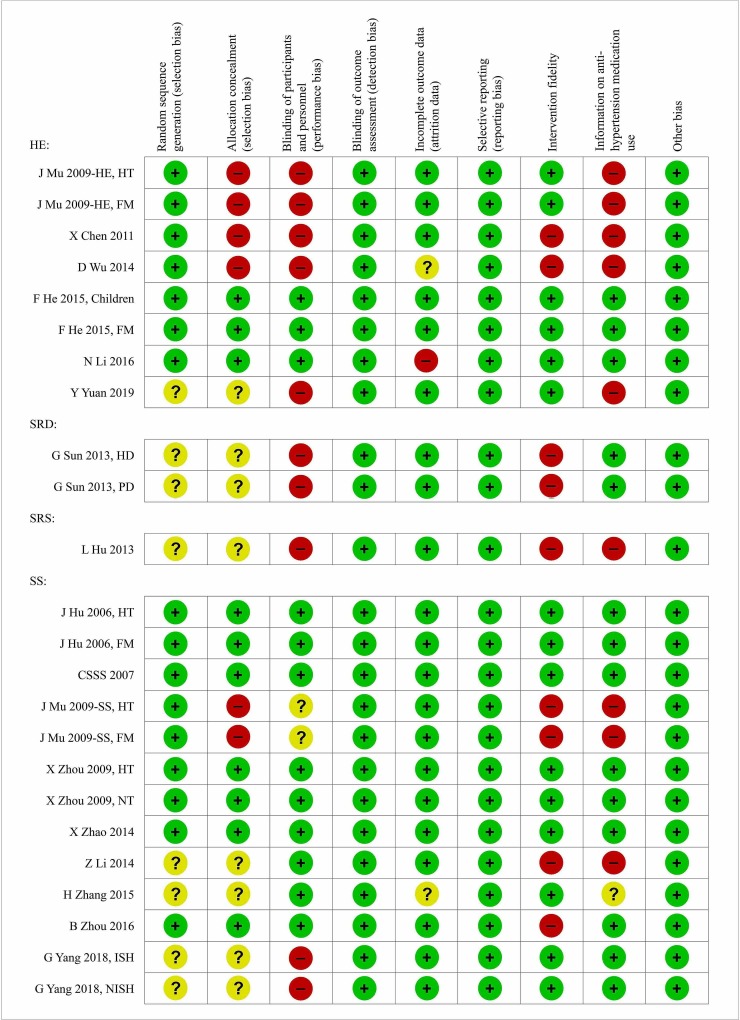
Data extraction and synthesis: Data were screened, extracted and appraised by two independent reviewers. The quality of study was assessed using a modified Cochrane Collaboration's risk of bias tool. The primary outcome was the difference in BP change from baseline to the end of study between interventions and control. The effects were pooled using a random effects model and associated factors were explored by a meta-regression.
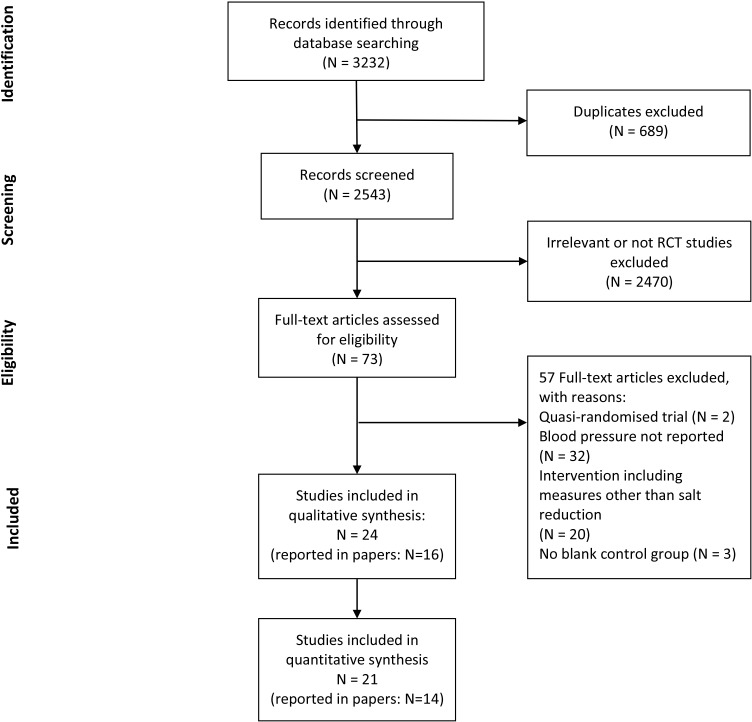
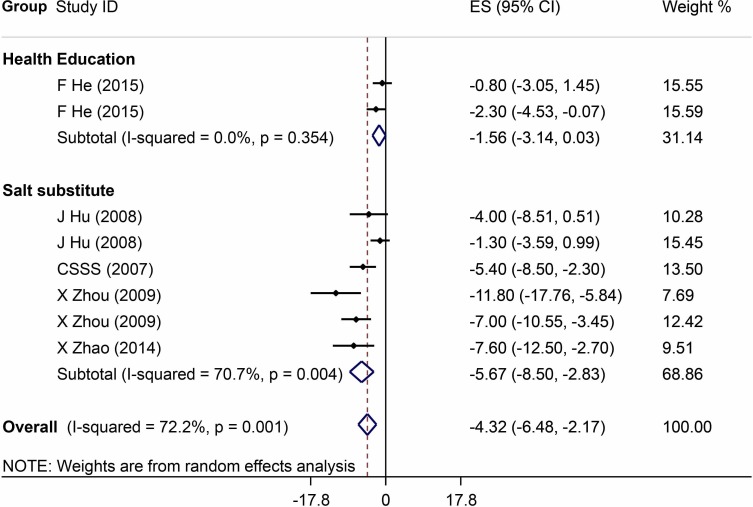
Results: We identified 24 studies involving 10 448 participants, including 8 studies on health education (4583 participants), 2 studies on salt restriction diet (162 participants), 1 study on salt restriction spoon (50 participants) and 13 studies on salt substitute (5653 participants). Six studies on salt substitute and three studies on health education were identified with high quality. Pooled results from the six studies showed that salt substitutes significantly reduced systolic BP (-5.7 mm Hg; 95% CI -8.5 to -2.8) and diastolic BP (-2.0 mm Hg; 95% CI -3.5 to -0.4). The School-EduSalt study showed that the school-based health education significantly reduced systolic BP among parents (-2.3 mm Hg; 95% CI -4.5 to -0.04).
Conclusions: Among four salt reduction strategies studied in China with RCT design, only salt substitute was proved effective in lowering BP by the pooled effect from multiple studies with high quality. More well-designed studies are warranted for other strategies.
Keywords: hypertension; nutrition & dietetics; public health.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: YW has received a small research fund from Chongqing Jiankangyuan Health Technology to study the effect of a new salt substitute with very low sodium.
Figures

References
-
- Roth GA, Abate D, Abate KH, et al. . Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of disease study 2017. The Lancet 2018;392:1736–88. 10.1016/S0140-6736(18)32203-7 - DOI - PMC - PubMed
-
- Wang Z, Chen Z, Zhang L, et al. . Status of hypertension in China: results from the China hypertension survey, 2012-2015. Circulation 2018;137:2344–56. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical