

Practical guidance for the management of acute lymphoblastic leukemia in the adolescent and young adult population
- PMID: 32071710
- PMCID: PMC6997963
- DOI: 10.1177/2040620720903531
Practical guidance for the management of acute lymphoblastic leukemia in the adolescent and young adult population
Abstract
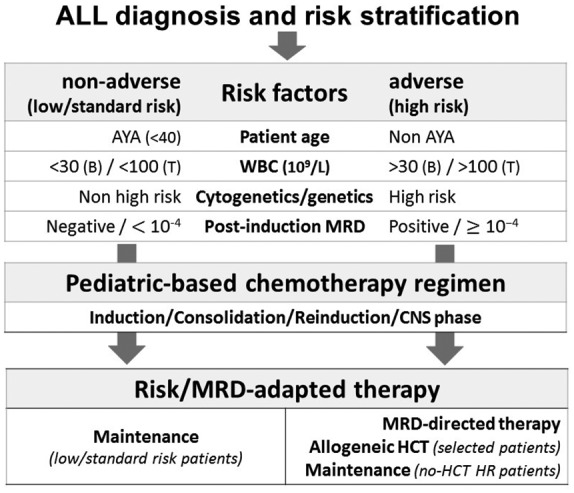
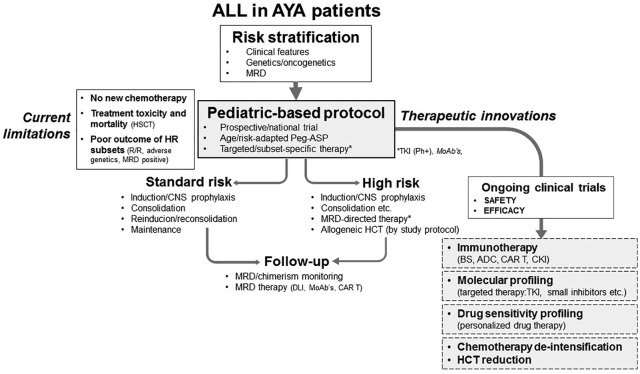
The outstanding therapeutic progress achieved with modern pediatric regimens in childhood acute lymphoblastic leukemia (ALL) led efforts to explore whether a similar treatment approach could be equally effective and safe in older patients, starting initially with older adolescents and young adults (AYA), variably defined in different studies by an age between 15-18 and 25-39 years. Several comparative and noncomparative trials of this type have been carried out during the last two decades, enrolling thousands of patients. Almost without exception, the new strategy improved patients' outcomes compared with traditional adult treatments in B-lineage and T-lineage Philadelphia (Ph) chromosome-negative B-ALL, while the use of tyrosine kinase inhibitors (TKI) led to comparative progress in Ph+ ALL, a former high-risk subset more typically observed in older age groups. At present, highly effective pediatric-based regimens warrant 5-year survival rates of 60-70% in AYA patients. In view of these data, the same approach was progressively extended to older patients, improving the results up to 55 years of age. Issues of treatment compliance and drug-related toxicity have thus far prevented a comparable therapeutic advancement in patients aged >55 years. This critical review updates and summarizes with pertinent examples this global, positive therapeutic change, and examines how to promote further progress with new targeted therapies that include novel immuno-therapeutics and other agents developed against the many molecular dysfunctions detectable in various ALL subsets. Substantial progress is expected to occur soon, bringing AYA survival figures very close to that of children, and also to improve the outcome of ALL at all ages.
Keywords: ALL; adolescent and young adults; therapy.
© The Author(s), 2020.
Conflict of interest statement
Conflict of interest statement: F. Carobolante, C. Skert: none; R. Bassan: fees, travel and accommodation expenses from Amgen, Pfizer, Shire, Servier, Incyte for consultancies and participation into boards and symposia; S. Chiaretti: fees, travel and accommodation expenses from Amgen, Pfizer, Shire, Incyte for consultancies and participation into boards and symposia.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
