

Complications after Radiofrequency Ablation for Hepatocellular Carcinoma: A Multicenter Study Involving 9,411 Japanese Patients
- PMID: 32071909
- PMCID: PMC7024979
- DOI: 10.1159/000502744
Complications after Radiofrequency Ablation for Hepatocellular Carcinoma: A Multicenter Study Involving 9,411 Japanese Patients
Abstract
Introduction: Radiofrequency ablation (RFA) for hepatocellular carcinoma (HCC) is considered a safe and minimally invasive procedure. We previously reported that the mortality and complication rates for RFA were 0.038% (5/13,283 patients) and 3.54% (579 complications/16,346 procedures), respectively, from 1999 to 2010 (previous period). In this study, we investigated the clinical criteria for RFA and the mortality and complication rates from 2011 to 2015 (recent period).
Methods: Data were collected from 25 centers by using a questionnaire developed by the Chugoku-Shikoku Society for Local Ablation Therapy of HCC. The criteria for RFA, RFA modification, use of image-guidance modalities, mortality, and complications during the previous and recent periods were compared.
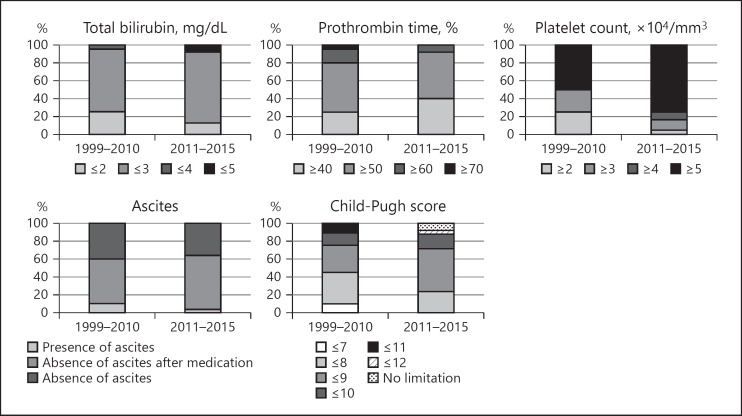
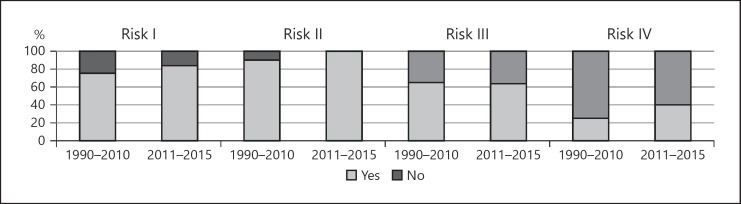
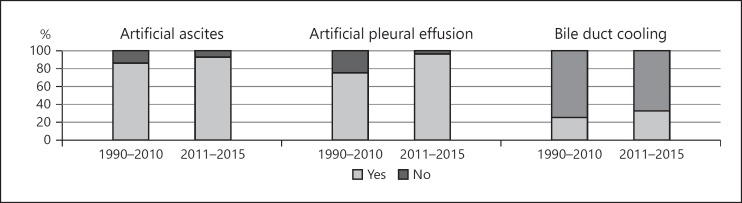
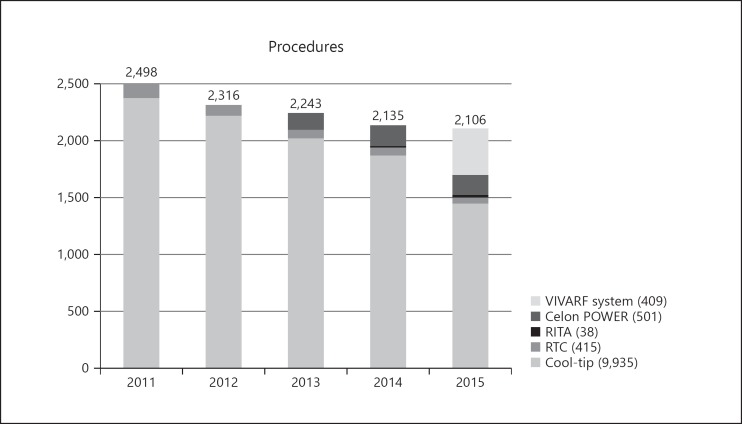
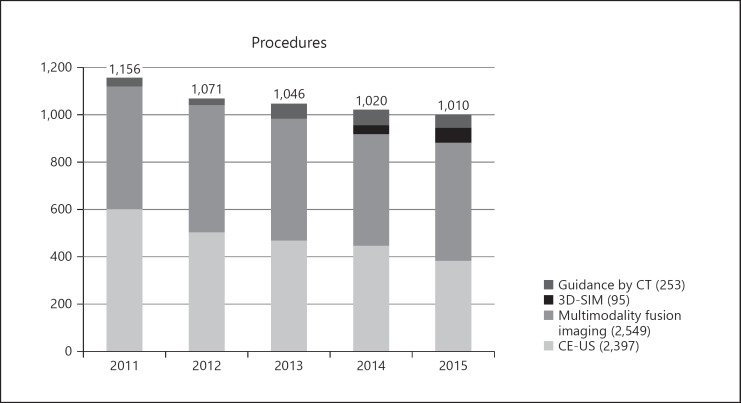
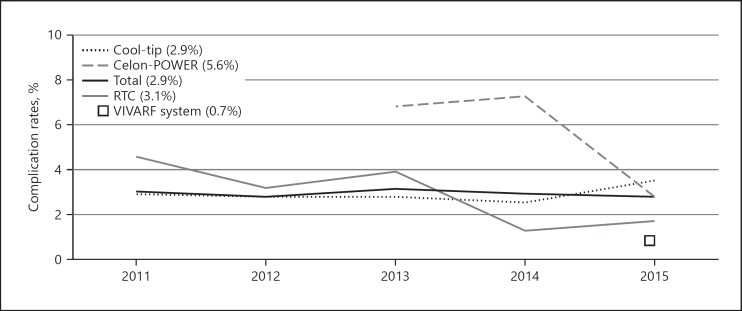
Results: We evaluated 11,298 procedures for 9,411 patients, including those that involved new devices (bipolar RFA and internally adjustable electrode system). The criterion of hepatic function for RFA increased from a Child-Pugh score ≤8 during the previous period to ≤9 during the recent period. The criteria regarding the tumor location and other risk factors have been expanded recently because of the increased use of several modifications of the RFA procedure and image-guidance modalities. The mortality rate was 0.064% (6/9,411 patients), and the complication rate was 2.92% (330 complications/11,298 procedures). There was no difference in mortality rates between the 2 periods (p = 0.38), but the complication rates was significantly lower during the recent period (p = 0.038).
Discussion and conclusions: Our findings confirmed that RFA, including the use of new devices, is a low-risk procedure for HCC, despite the expansion of the criteria for RFA during the recent period.
Keywords: Complication; Hepatocellular carcinoma; Mortality; Radiofrequency ablation.
Copyright © 2019 by S. Karger AG, Basel.
Conflict of interest statement
I. Sakaida: received funding from Otsuka and Gilead; K. Takaguchi: received funding from AbbVie KK, MSD, Bristol Myers Squibb, AstraZeneca KK, and Gilead; the other authors do not have any disclosures.
Figures
References
-
- GLOBOCAN 2018 Available from: http://globocan.iarc.fr/
-
- Kudo M, Izumi N, Ichida T, Ku Y, Kokudo N, Sakamoto M, et al. Report of the 19th follow-up survey of primary liver cancer in Japan. Hepatol Res. 2016 Mar;46((5)):372–90. - PubMed
-
- Livraghi T, Solbiati L, Meloni MF, Gazelle GS, Halpern EF, Goldberg SN. Treatment of focal liver tumors with percutaneous radio-frequency ablation: complications encountered in a multicenter study. Radiology. 2003 Feb;226((2)):441–51. - PubMed
-
- de Baère T, Risse O, Kuoch V, Dromain C, Sengel C, Smayra T, et al. Adverse events during radiofrequency treatment of 582 hepatic tumors. AJR Am J Roentgenol. 2003 Sep;181((3)):695–700. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
