

TXA (Tranexamic Acid) Risk Evaluation in Combat Casualties (TRECC)
- PMID: 32072015
- PMCID: PMC6996783
- DOI: 10.1136/tsaco-2019-000353
TXA (Tranexamic Acid) Risk Evaluation in Combat Casualties (TRECC)
Abstract
Background: The use of tranexamic acid (TXA) has become increasingly prevalent for hemorrhage prevention in military trauma patients due to its known survival benefits. There is concern of increased venous thromboembolism (VTE) subsequent to receiving TXA. The purpose of this retrospective study was to determine the rate of VTE in severely injured military personnel during Operation Enduring Freedom (2009-2014).
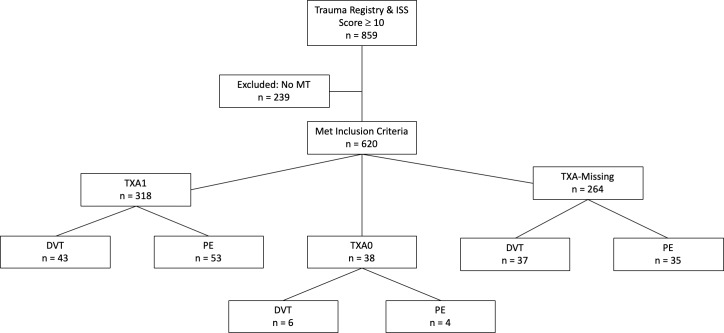
Methods: An analysis of 859 military trauma patients from the 2009-2014 Department of Defense Trauma Registry included subjects with an injury severity score (ISS) >10 and a massive transfusion (MT) (>10 units of blood products in the first 24 hours). Outcomes included a documented VTE (eg, deep vein thrombosis (DVT) or pulmonary embolism (PE)) during the patient's hospital course. Comparison between those who did/did not receive TXA was analyzed using three separate multiple regression analyses using listwise deletion, systematic replacement and multiple imputation.
Results: Subjects (n=620) met inclusion criteria with 27% (n=169) having a documented VTE. A total of 30% that received TXA had a documented VTE, 26% that did not receive TXA had a documented VTE and 43% (n=264, n=620) of the sample did not have TXA documented as either given or not given. Multiple regression analyses using listwise deletion and systematic replacement of the TXA variable demonstrated no difference in odds of VTE, whereas the multiple imputation analysis demonstrated a 3% increased odds of VTE, a9.4% increased odds of PE and 8.1% decreased odds of DVT with TXA administration.
Discussion: TXA use with an ISS >10 and MT resuscitation had a 3% increased odds of VTE and an increased odds of PE, whereas the odds of DVT were found to be decreased after multiple imputation analysis. Further research on the long-term risks and benefits of TXA usage in the military population is recommended.
Level of evidence: IV-therapeutic.
Keywords: deep vein thrombosis; pulmonary embolism; surgery; tranexamic acid; trauma.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous