

Pediatric pain treatment and prevention for hospitalized children
- PMID: 32072099
- PMCID: PMC7004501
- DOI: 10.1097/PR9.0000000000000804
Pediatric pain treatment and prevention for hospitalized children
Abstract
Introduction: Prevention and treatment of pain in pediatric patients compared with adults is often not only inadequate but also less often implemented the younger the children are. Children 0 to 17 years are a vulnerable population.
Objectives: To address the prevention and treatment of acute and chronic pain in children, including pain caused by needles, with recommended analgesic starting doses.
Methods: This Clinical Update elaborates on the 2019 IASP Global Year Against Pain in the Vulnerable "Factsheet Pain in Children: Management" and reviews best evidence and practice.
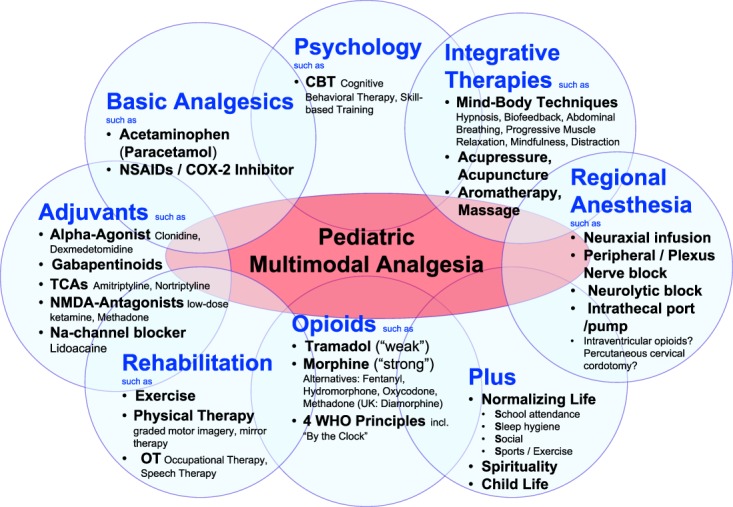
Results: Multimodal analgesia may include pharmacology (eg, basic analgesics, opioids, and adjuvant analgesia), regional anesthesia, rehabilitation, psychological approaches, spirituality, and integrative modalities, which act synergistically for more effective acute pediatric pain control with fewer side effects than any single analgesic or modality. For chronic pain, an interdisciplinary rehabilitative approach, including physical therapy, psychological treatment, integrative mind-body techniques, and normalizing life, has been shown most effective. For elective needle procedures, such as blood draws, intravenous access, injections, or vaccination, overwhelming evidence now mandates that a bundle of 4 modalities to eliminate or decrease pain should be offered to every child every time: (1) topical anesthesia, eg, lidocaine 4% cream, (2) comfort positioning, eg, skin-to-skin contact for infants, not restraining children, (3) sucrose or breastfeeding for infants, and (4) age-appropriate distraction. A deferral process (Plan B) may include nitrous gas analgesia and sedation.
Conclusion: Failure to implement evidence-based pain prevention and treatment for children in medical facilities is now considered inadmissible and poor standard of care.
Keywords: Breastfeeding; Comfort positioning; Distraction; Multimodal analgesia; Pain prevention; Pain treatment; Pediatric pain; Sucrose; Topical anesthesia.
Copyright © 2019 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The International Association for the Study of Pain.
Conflict of interest statement
The authors have no conflicts of interest to declare.Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
References
-
- American Society of Anesthesiologists Task Force on S, Analgesia by N-A. Practice guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology 2002;96:1004–17. - PubMed
-
- Anand KJ, Barton BA, McIntosh N, Lagercrantz H, Pelausa E, Young TE, Vasa R. Analgesia and sedation in preterm neonates who require ventilatory support: results from the NOPAIN trial. Neonatal outcome and prolonged analgesia in neonates. Arch Pediatr Adolesc Med 1999;153:331–8. - PubMed
-
- Baeumler PI, Fleckenstein J, Benedikt F, Bader J, Irnich D. Acupuncture-induced changes of pressure pain threshold are mediated by segmental inhibition—a randomized controlled trial. PAIN 2015;156:2245–55. - PubMed
-
- Benoit B, Campbell-Yeo M, Johnston C, Latimer M, Caddell K, Orr T. Staff nurse utilization of kangaroo care as an intervention for procedural pain in preterm infants. Adv Neonatal Care 2016;16:229–38. - PubMed
-
- Beyer JE, DeGood DE, Ashley LC, Russell GA. Patterns of postoperative analgesic use with adults and children following cardiac surgery. PAIN 1983;17:71–81. - PubMed
LinkOut - more resources
Full Text Sources
Medical