

Insight Into the Posthospital Syndrome: A 3-Month Longitudinal Follow up on Geriatric Syndromes and Their Association With Functional Decline, Readmission, and Mortality
- PMID: 32072168
- PMCID: PMC7302165
- DOI: 10.1093/gerona/glaa039
Insight Into the Posthospital Syndrome: A 3-Month Longitudinal Follow up on Geriatric Syndromes and Their Association With Functional Decline, Readmission, and Mortality
Abstract
Background: Acute hospitalization may lead to posthospital syndrome, but no studies have investigated how this syndrome manifests and geriatric syndromes are often used as synonym. However, studies on longitudinal associations between syndromes and adverse outcomes are scarce. We aimed to analyze longitudinal associations between geriatric syndromes and functional decline (FD), readmission, and mortality.
Methods: Prospective cohort study, including 401 acutely hospitalized patients (aged ≥ 70). We performed: (i) logistic regression analyses to assess associations between patterns of geriatric syndromes as they develop over time (between admission and 1 month postdischarge), and FD and readmission; (ii) generalized estimating equations to assess longitudinal associations between geriatric syndromes over five time points (admission, discharge, 1, 2, and 3 months postdischarge) and FD, mortality, and readmission at 3 months postdischarge.
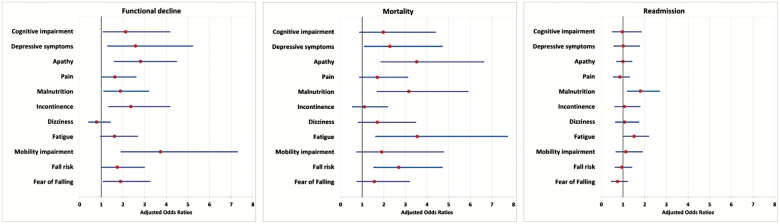
Results: After syndrome absent, syndrome present at both admission and 1 month postdischarge was most prevalent. Persistent patterns of apathy (odds ratio [OR] = 4.35, 95% confidence interval [CI] = 1.54-12.30), pain (OR = 3.26, 95% CI = 1.21-8.8), malnutrition (OR = 3.4, 95% CI = 1.35-8.56), mobility impairment (OR = 6.65, 95% CI = 1.98-22.38), and fear of falling (OR = 3.17, 95% CI = 1.25-8.02) were associated with FD. Developing cognitive impairment (OR = 6.40, 95% CI = 1.52-26.84), fatigue (OR = 4.71, 95% CI = 1.03-21.60), and fall risk (OR = 4.30, 95% CI = 1.21-16.57) postdischarge, was associated with readmission; however, only 4%-6% developed these syndromes. Over the course of five time points, mobility impairment, apathy, and incontinence were longitudinally associated with FD; apathy, malnutrition, fatigue, and fall risk with mortality; malnutrition with readmission.
Conclusion: Most geriatric syndromes are present at admission and patients are likely to retain them postdischarge. Several geriatric syndromes are longitudinally associated with mortality and, particularly, persistently present syndromes place persons are at risk of FD. Although few persons develop syndromes postdischarge, those developing cognitive impairment, fatigue, and fall risk were at increased readmission risk.
Keywords: Geriatric syndromes; Acute hospitalization; Adverse outcomes; Postdischarge.
© The Author(s) 2020. Published by Oxford University Press on behalf of The Gerontological Society of America.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
