

Brain tumour diagnostics using a DNA methylation-based classifier as a diagnostic support tool
- PMID: 32072658
- PMCID: PMC7496466
- DOI: 10.1111/nan.12610
Brain tumour diagnostics using a DNA methylation-based classifier as a diagnostic support tool
Abstract
Aims: Methylation profiling (MP) is increasingly incorporated in the diagnostic process of central nervous system (CNS) tumours at our centres in The Netherlands and Scandinavia. We aimed to identify the benefits and challenges of MP as a support tool for CNS tumour diagnostics.
Methods: About 502 CNS tumour samples were analysed using (850 k) MP. Profiles were matched with the DKFZ/Heidelberg CNS Tumour Classifier. For each case, the final pathological diagnosis was compared to the diagnosis before MP.
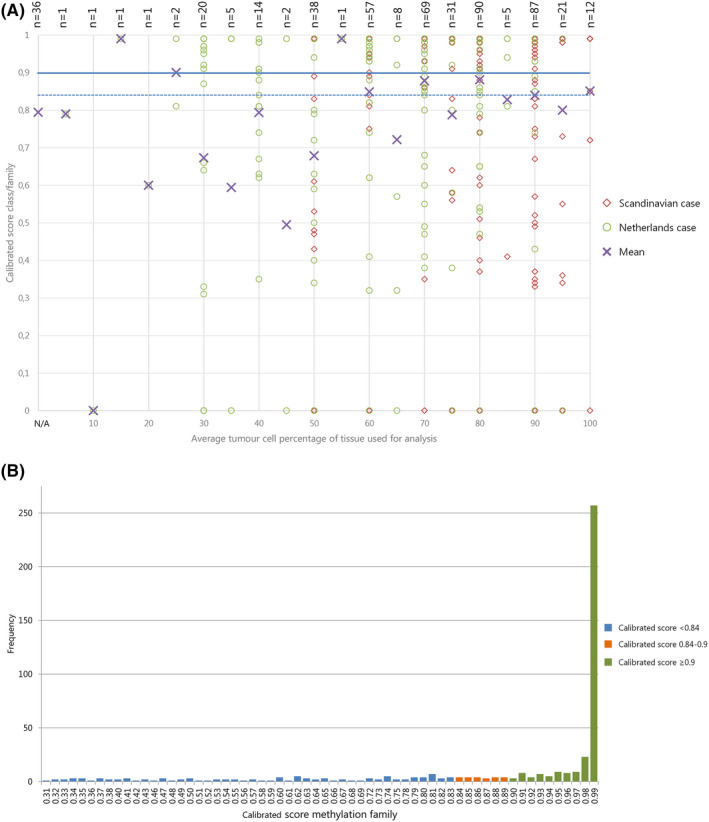
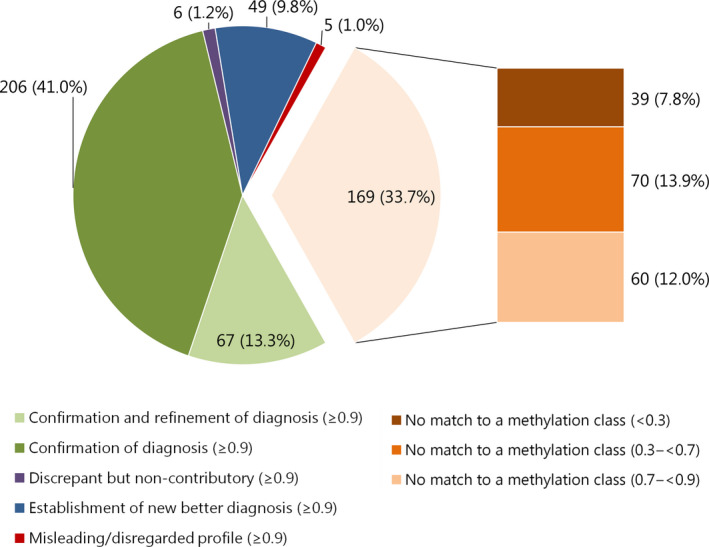
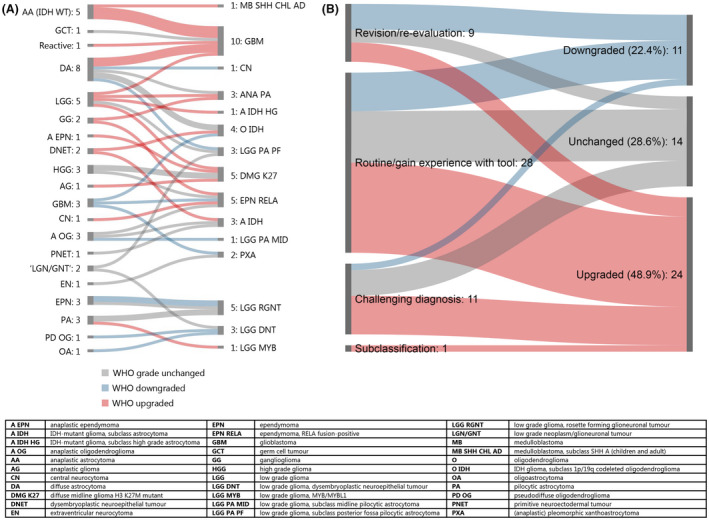
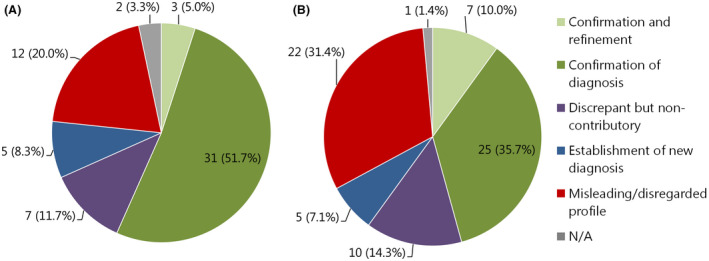
Results: In 54.4% (273/502) of all analysed cases, the suggested methylation class (calibrated score ≥0.9) corresponded with the initial pathological diagnosis. The diagnosis of 24.5% of these cases (67/273) was more refined after incorporation of the MP result. In 9.8% of cases (49/502), the MP result led to a new diagnosis, resulting in an altered WHO grade in 71.4% of these cases (35/49). In 1% of cases (5/502), the suggested class based on MP was initially disregarded/interpreted as misleading, but in retrospect, the MP result predicted the right diagnosis for three of these cases. In six cases, the suggested class was interpreted as 'discrepant but noncontributory'. The remaining 33.7% of cases (169/502) had a calibrated score <0.9, including 7.8% (39/502) for which no class indication was given at all (calibrated score <0.3).
Conclusions: MP is a powerful tool to confirm and fine-tune the pathological diagnosis of CNS tumours, and to avoid misdiagnoses. However, it is crucial to interpret the results in the context of clinical, radiological, histopathological and other molecular information.
Keywords: central nervous system tumours; diagnostics; methylation profiling.
© 2020 The Authors. Neuropathology and Applied Neurobiology published by John Wiley & Sons Ltd on behalf of British Neuropathological Society.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Kros JM, Gorlia T, Kouwenhoven MC, Zheng P, Collins VP, Figarella‐branger D et al Panel review of anaplastic oligodendroglioma from European organization for research and treatment of cancer trial 26951: assessment of consensus in diagnosis, influence of 1p/19q Loss, and correlations with outcome. J Neuropathol Exp Neurol 2007; 66: 545–51 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
