

Endothelial dysfunction is an early indicator of sepsis and neutrophil degranulation of septic shock in surgical patients
- PMID: 32073224
- PMCID: PMC7260414
- DOI: 10.1002/bjs5.50265
Endothelial dysfunction is an early indicator of sepsis and neutrophil degranulation of septic shock in surgical patients
Abstract
Background: Stratification of the severity of infection is currently based on the Sequential Organ Failure Assessment (SOFA) score, which is difficult to calculate outside the ICU. Biomarkers could help to stratify the severity of infection in surgical patients.
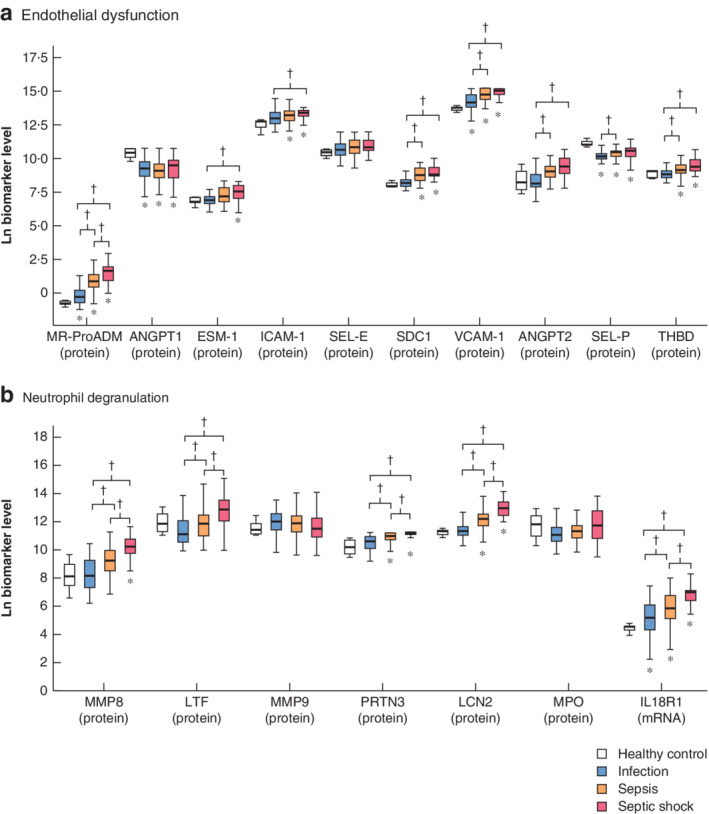
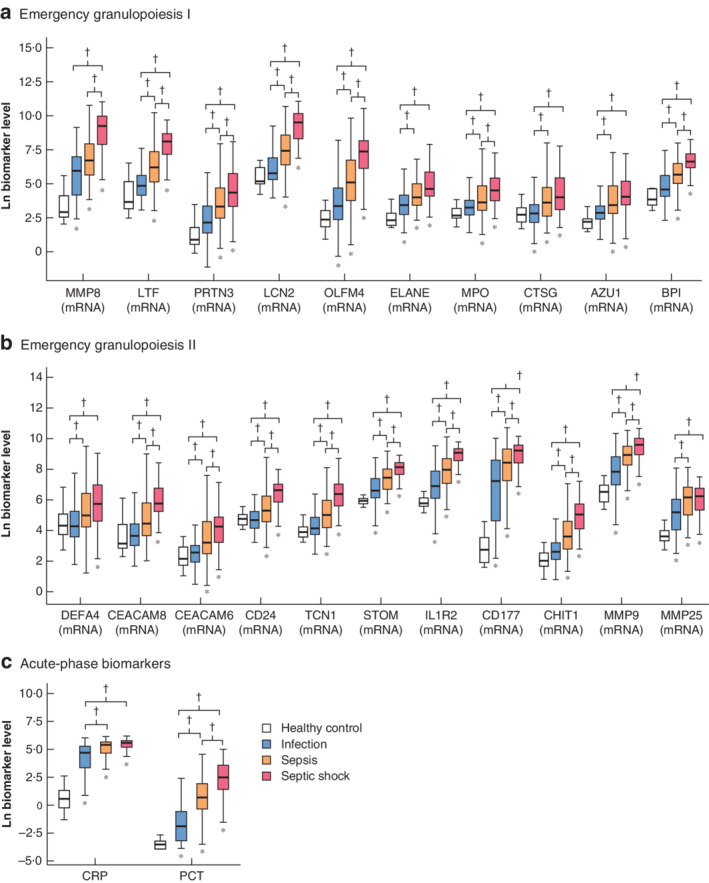
Methods: Levels of ten biomarkers indicating endothelial dysfunction, 22 indicating emergency granulopoiesis, and six denoting neutrophil degranulation were compared in three groups of patients in the first 12 h after diagnosis at three Spanish hospitals.
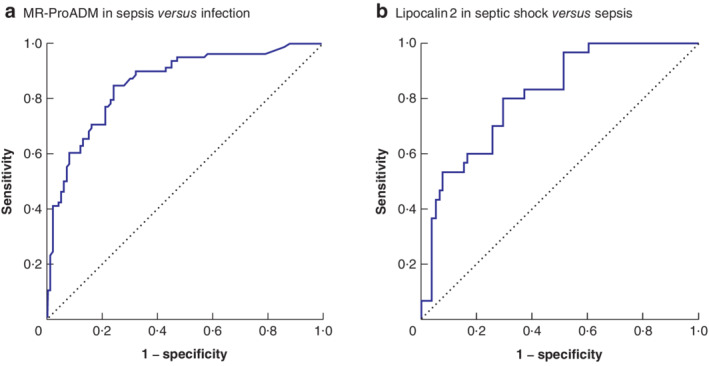
Results: There were 100 patients with infection, 95 with sepsis and 57 with septic shock. Seven biomarkers indicating endothelial dysfunction (mid-regional proadrenomedullin (MR-ProADM), syndecan 1, thrombomodulin, angiopoietin 2, endothelial cell-specific molecule 1, vascular cell adhesion molecule 1 and E-selectin) had stronger associations with sepsis than infection alone. MR-ProADM had the highest odds ratio (OR) in multivariable analysis (OR 11·53, 95 per cent c.i. 4·15 to 32·08; P = 0·006) and the best area under the curve (AUC) for detecting sepsis (0·86, 95 per cent c.i. 0·80 to 0·91; P < 0·001). In a comparison of sepsis with septic shock, two biomarkers of neutrophil degranulation, proteinase 3 (OR 8·09, 1·34 to 48·91; P = 0·028) and lipocalin 2 (OR 6·62, 2·47 to 17·77; P = 0·002), had the strongest association with septic shock, but lipocalin 2 exhibited the highest AUC (0·81, 0·73 to 0·90; P < 0·001).
Conclusion: MR-ProADM and lipocalin 2 could be alternatives to the SOFA score in the detection of sepsis and septic shock respectively in surgical patients with infection.
Antecedentes: La estratificación de la gravedad de una infección se basa actualmente en la puntuación SOFA (Sequential Organ Failure Assessment), que es difícil de calcular fuera de la unidad de cuidados intensivos. Los biomarcadores podrían ayudar a estratificar la gravedad de la infección en pacientes quirúrgicos. MÉTODOS: Se compararon las concentraciones de 10 biomarcadores que denotan disfunción endotelial, 22 que indican granulopoyesis de emergencia y 6 que expresan la degranulación de neutrófilos en tres grupos de pacientes de tres hospitales españoles (100 con infección, 95 con sepsis y 57 con shock séptico) en las primeras doce horas después del diagnóstico.
Resultados: Siete biomarcadores que expresan disfunción endotelial (proadrenomedulina, sindecan-1, trombomodulina, angiopoyetina-2, endocan-1, molécula de adhesión endotelial 1 y E-selectina) mostraron una fuerte asociación con la sepsis en comparación con la infección aislada. La proadrenomedulina presentó el valor más alto de la razón de oportunidades (odds ratio, OR) en el análisis multivariable (OR 11,53, i.c. del 95% 4,15-32,08, P = 0,006) y la mejor área bajo la curva para detectar sepsis (AUC 0,86, i.c. del 95% 0,80-0,91, P < 0,001). En la comparación entre sepsis y shock séptico, los biomarcadores que mostraron la asociación más estrecha con el shock séptico fueron dos biomarcadores de degranulación de neutrófilos (proteinasa-3 y lipocalina-2) (OR 8,09, i.c. del 9% 1,34-48,91, P = 0,028; OR 6.62, i.c. del 95% 2,47-17,77, P = 0,002), pero la lipocalina-2 presentó la mejor AUC (0,81, i.c. del 95% 0,73-0,90, P < 0,001). CONCLUSIÓN: la proadrenomedulina y la lipocalina-2 podrían representar alternativas a la puntuación SOFA para detectar sepsis y shock séptico en pacientes quirúrgicos con infección.
© 2020 The Authors. BJS Open published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures
References
-
- Angus DC, Linde‐Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 2001; 29: 1303–1310. - PubMed
-
- Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H et al The SOFA (Sepsis‐related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis‐Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med 1996; 22: 707–710. - PubMed
-
- Serafim R, Gomes JA, Salluh J, Póvoa P. A Comparison of the quick‐SOFA and systemic inflammatory response syndrome criteria for the diagnosis of sepsis and prediction of mortality: a systematic review and meta‐analysis. Chest 2018; 153: 646–655. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- Consejería de Educación de Castilla y León/Fondo social Europeo/International
- European Union (Fondo Europeo de Desarrollo Regional, Una manera de hacer Europa)/International
- PI15/01451/Instituto de Salud Carlos III/International
- PI15/01959/Instituto de Salud Carlos III/International
- PI16/01156/Instituto de Salud Carlos III/International
LinkOut - more resources
Full Text Sources
Medical
