

Olaparib Versus Nonplatinum Chemotherapy in Patients With Platinum-Sensitive Relapsed Ovarian Cancer and a Germline BRCA1/2 Mutation (SOLO3): A Randomized Phase III Trial
- PMID: 32073956
- PMCID: PMC7145583
- DOI: 10.1200/JCO.19.02745
Olaparib Versus Nonplatinum Chemotherapy in Patients With Platinum-Sensitive Relapsed Ovarian Cancer and a Germline BRCA1/2 Mutation (SOLO3): A Randomized Phase III Trial
Abstract
Purpose: A phase II study (ClinicalTrials.gov identifier: NCT00628251) showed activity of olaparib capsules versus pegylated liposomal doxorubicin in patients with germline BRCA-mutated platinum-resistant or partially platinum-sensitive relapsed ovarian cancer. We conducted a phase III trial (SOLO3) of olaparib tablets versus nonplatinum chemotherapy in patients with germline BRCA-mutated platinum-sensitive relapsed ovarian cancer who had received at least 2 prior lines of platinum-based chemotherapy.
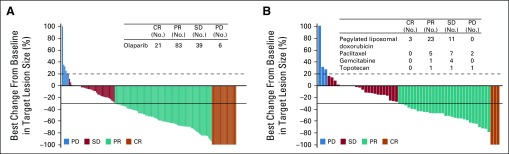
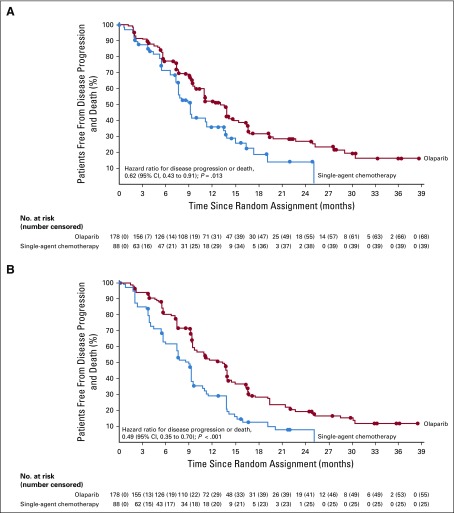
Patients and methods: In this randomized, open-label trial, patients were randomly assigned 2:1 to olaparib 300 mg twice a day or physician's choice single-agent nonplatinum chemotherapy (pegylated liposomal doxorubicin, paclitaxel, gemcitabine, or topotecan). The primary end point was objective response rate (ORR) in the measurable disease analysis set assessed by blinded independent central review (BICR). The key secondary end point was progression-free survival (PFS) assessed by BICR in the intent-to-treat population.
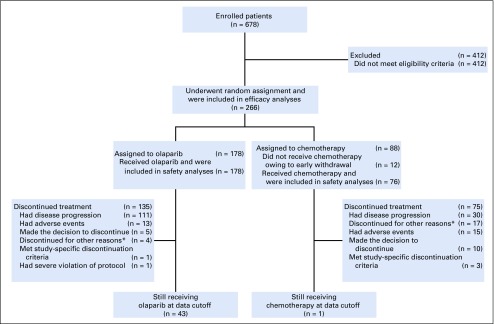
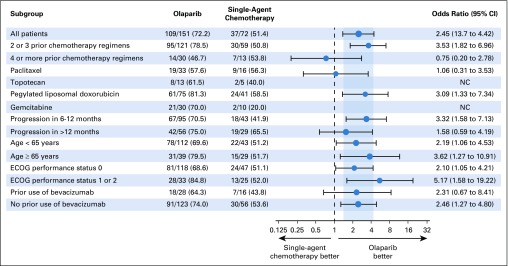
Results: Of 266 randomly assigned patients, 178 were assigned to olaparib and 88 to chemotherapy. In patients with measurable disease (olaparib, n = 151; chemotherapy, n = 72), the BICR-assessed ORR was significantly higher with olaparib than with chemotherapy (72.2% v 51.4%; odds ratio [OR], 2.53 [95% CI, 1.40 to 4.58]; P = .002). In the subgroup who had received 2 prior lines of treatment, the ORR was 84.6% with olaparib and 61.5% with chemotherapy (OR, 3.44 [95% CI, 1.42 to 8.54]). BICR-assessed PFS also significantly favored olaparib versus chemotherapy (hazard ratio, 0.62 [95% CI, 0.43 to 0.91]; P = .013; median, 13.4 v 9.2 months). Adverse events were consistent with the established safety profiles of olaparib and chemotherapy.
Conclusion: Olaparib resulted in statistically significant and clinically relevant improvements in ORR and PFS compared with nonplatinum chemotherapy in patients with germline BRCA-mutated platinum-sensitive relapsed ovarian cancer who had received at least 2 prior lines of platinum-based chemotherapy.
Trial registration: ClinicalTrials.gov NCT00628251 NCT02282020.
Figures
Comment in
-
Reply to E. Paulino et al.J Clin Oncol. 2020 Aug 10;38(23):2698. doi: 10.1200/JCO.20.01235. Epub 2020 Jun 12. J Clin Oncol. 2020. PMID: 32530766 No abstract available.
-
SOLO 3 Trial: How Do the Results Fit in With Current Evidence?J Clin Oncol. 2020 Aug 10;38(23):2697-2698. doi: 10.1200/JCO.20.00576. Epub 2020 Jun 12. J Clin Oncol. 2020. PMID: 32530768 No abstract available.
References
-
- O’Connor MJ. Targeting the DNA damage response in cancer. Mol Cell. 2015;60:547–560. - PubMed
-
- Matulonis UA, Penson RT, Domchek SM, et al. Olaparib monotherapy in patients with advanced relapsed ovarian cancer and a germline BRCA1/2 mutation: A multistudy analysis of response rates and safety. Ann Oncol. 2016;27:1013–1019. - PubMed
-
- Fong PC, Boss DS, Yap TA, et al. Inhibition of poly(ADP-ribose) polymerase in tumors from BRCA mutation carriers. N Engl J Med. 2009;361:123–134. - PubMed
-
- Fong PC, Yap TA, Boss DS, et al. Poly(ADP)-ribose polymerase inhibition: Frequent durable responses in BRCA carrier ovarian cancer correlating with platinum-free interval. J Clin Oncol. 2010;28:2512–2519. - PubMed
-
- Mateo J, Moreno V, Gupta A, et al. An adaptive study to determine the optimal dose of the tablet formulation of the PARP inhibitor olaparib. Target Oncol. 2016;11:401–415. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
