

New Biopsy Techniques and Imaging Features of Transrectal Ultrasound for Targeting PI-RADS 4 and 5 Lesions
- PMID: 32075275
- PMCID: PMC7073696
- DOI: 10.3390/jcm9020530
New Biopsy Techniques and Imaging Features of Transrectal Ultrasound for Targeting PI-RADS 4 and 5 Lesions
Abstract
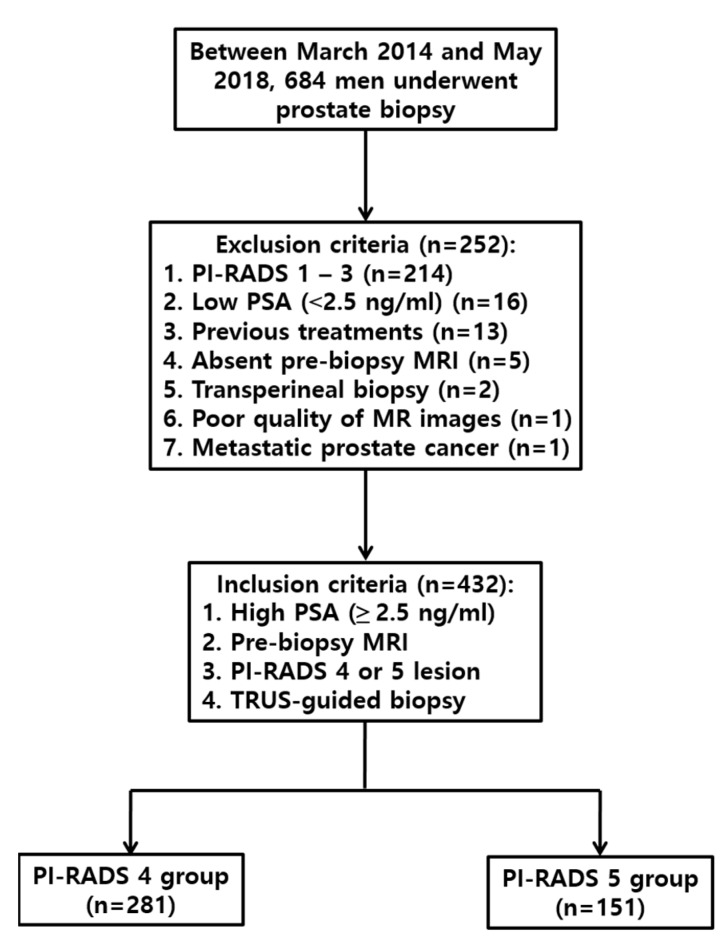
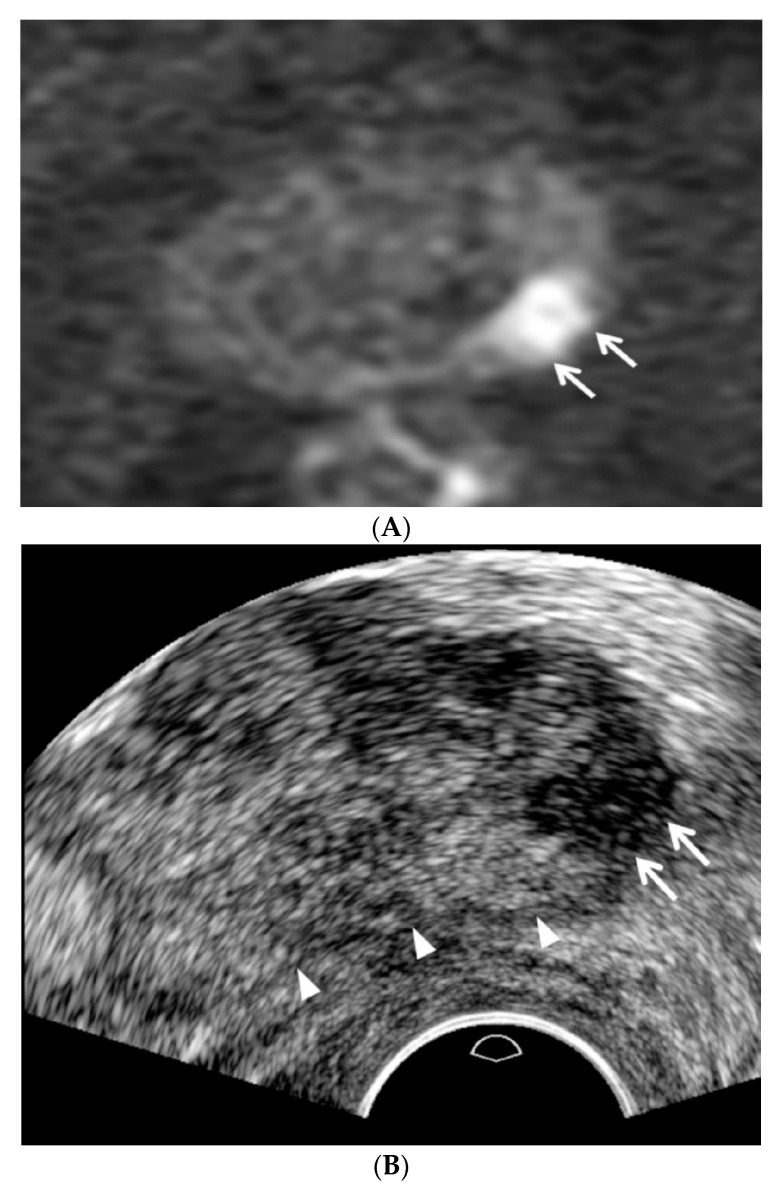
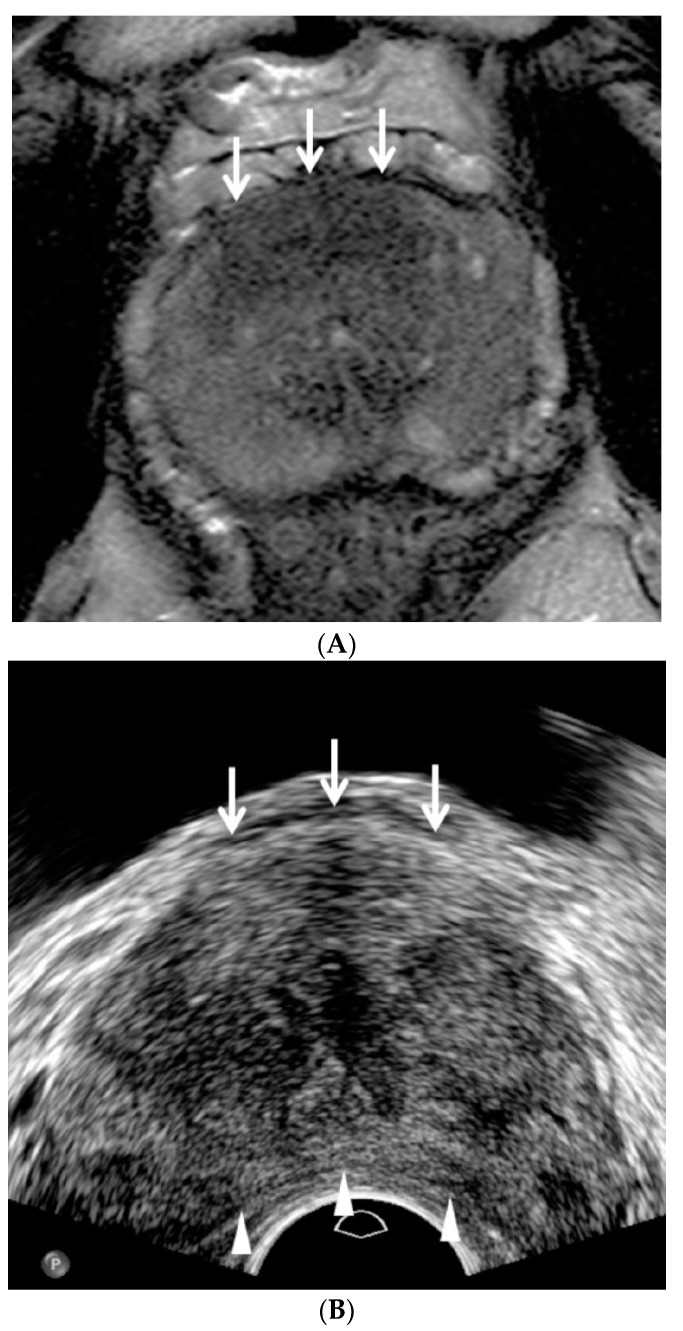
Purpose: To introduce new biopsy techniques and imaging features of transrectal ultrasound (TRUS) for targeting Prostate Imaging Reporting and Data System (PI-RADS) 4 and 5 lesions Methods: TRUS-guided targeted and/or systematic biopsies were performed in 432 men with PI-RADS 4 and 5 lesions following magnetic resonance imaging examination. A TRUS operator who was familiar with the new techniques and imaging features performed lesion detection. Overall and significant cancer detection rates (CDRs) were compared among the men with PI-RADS 4 and 5 lesions. The CDRs in the peripheral and transition zones were compared. Additionally, we assessed whether targeted or systematic biopsies contributed to cancer detection. The standard reference was a biopsy examination.
Results: The overall CDRs in the men with PI-RADS 4 and 5 lesions were 49.5% (139/281) and 74.8% (113/151) (p < 0.0001); significant CDRs were 33.1% (93/281) and 58.3% (88/151) (p < 0.0001); and CDRs in the peripheral and transition zones were 53.6% (187/349) and 78.3% (65/83) (p < 0.0001), respectively. Of the 139 men with clinically significant cancer PI-RADS 4 lesions, 107 (77.0%) were diagnosed by targeted biopsy, 5 (3.6%) by systematic biopsy, and 27 (19.4%) by both. Of the 113 men with clinically significant cancer PI-RADS 5 lesions, 97 (85.8%) were diagnosed by targeted biopsy, 3 (2.7%) by systematic biopsy, and 13 (11.5%) by both.
Conclusions: Most PI-RADS 4 and 5 lesions can be targeted with TRUS if the new techniques and imaging features are applied.
Keywords: Prostate Imaging Reporting and Data System; biopsy; magnetic resonance imaging; prostate adenocarcinoma; transrectal ultrasound.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Transrectal ultrasound features and biopsy outcomes of transition PI-RADS 5.Acta Radiol. 2022 Apr;63(4):559-565. doi: 10.1177/02841851211018775. Epub 2021 May 22. Acta Radiol. 2022. PMID: 34027681
-
Multiparametric magnetic resonance imaging - Transrectal ultrasound-guided cognitive fusion biopsy of the prostate: Clinically significant cancer detection rates stratified by the Prostate Imaging and Data Reporting System version 2 assessment category.Can Urol Assoc J. 2018 Dec;12(12):401-406. doi: 10.5489/cuaj.5254. Can Urol Assoc J. 2018. PMID: 29940139 Free PMC article.
-
Targeted MRI/TRUS fusion-guided biopsy in men with previous prostate biopsies using a novel registration software and multiparametric MRI PI-RADS scores: first results.World J Urol. 2015 Nov;33(11):1707-14. doi: 10.1007/s00345-015-1525-4. Epub 2015 Mar 14. World J Urol. 2015. PMID: 25774003
-
Multiparametric MRI in detection and staging of prostate cancer.Dan Med J. 2017 Feb;64(2):B5327. Dan Med J. 2017. PMID: 28157066 Review.
-
How to Improve TRUS-Guided Target Biopsy following Prostate MRI.Cancers (Basel). 2021 Nov 11;13(22):5647. doi: 10.3390/cancers13225647. Cancers (Basel). 2021. PMID: 34830798 Free PMC article. Review.
Cited by
-
Current Approach to Complications and Difficulties during Transrectal Ultrasound-Guided Prostate Biopsies.J Clin Med. 2024 Jan 16;13(2):487. doi: 10.3390/jcm13020487. J Clin Med. 2024. PMID: 38256621 Free PMC article. Review.
-
New transperineal ultrasound-guided biopsy for men in whom PSA is increasing after Miles' operation.Insights Imaging. 2023 Mar 16;14(1):42. doi: 10.1186/s13244-023-01384-y. Insights Imaging. 2023. PMID: 36929129 Free PMC article.
-
TRUS-Guided Target Biopsy for a PI-RADS 3-5 Index Lesion to Reduce Gleason Score Underestimation: A Propensity Score Matching Analysis.Front Oncol. 2022 Jan 24;11:824204. doi: 10.3389/fonc.2021.824204. eCollection 2021. Front Oncol. 2022. PMID: 35141158 Free PMC article.
-
Research progress on deep learning in magnetic resonance imaging-based diagnosis and treatment of prostate cancer: a review on the current status and perspectives.Front Oncol. 2023 Jun 13;13:1189370. doi: 10.3389/fonc.2023.1189370. eCollection 2023. Front Oncol. 2023. PMID: 37546423 Free PMC article. Review.
-
New TRUS Techniques and Imaging Features of PI-RADS 4 or 5: Influence on Tumor Targeting.Front Oncol. 2021 Jun 9;11:608409. doi: 10.3389/fonc.2021.608409. eCollection 2021. Front Oncol. 2021. PMID: 34178615 Free PMC article.
References
-
- Hernandez A.D., Smith J.A., Jr. Transrectal ultrasonography for the early detection and staging of prostate cancer. Urol. Clin. N. Am. 1990;17:745–757. - PubMed
-
- Zackrisson B., Aus G., Bergdahl S., Lilja H., Lodding P., Pihl C.G., Hugosson J. The risk of finding focal cancer (less than 3 mm) remains high on re-biopsy of patients with persistently increased prostate specific antigen but the clinical significance is questionable. J. Urol. 2004;171:1500–1503. doi: 10.1097/01.ju.0000118052.59597.83. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
