

Rectal aberrant crypt foci (ACF) as a predictor of benign and malignant neoplastic lesions in the large intestine
- PMID: 32075595
- PMCID: PMC7029492
- DOI: 10.1186/s12885-020-6590-4
Rectal aberrant crypt foci (ACF) as a predictor of benign and malignant neoplastic lesions in the large intestine
Abstract
Background: The importance of ACF is not fully explained, however, their number may be a good predictor of synchronous and metachronic adenoma or other polyps whose removal reduces the risk of CRC. Due to the epidemiological and genetic association of ACF with pre-cancer lesions, they may be a potential CRC biomarker. The aim of our study was to show that the number and type of rectal ACF may be a good predictive factor for the presence of polyps located proximally from the splenic flexure and that the type and number of ACF can correlate with the number and specific types of polyps in the large intestine.
Methods: The study included 131 patients who underwent colonoscopy combined with rectal mucosa staining with 0.25% methylene blue. The number of rectal ACF was determined and bioptats were sampled for histopathological examination to assess the type of ACF. Endoscopic ACF assessment criteria given by L. Roncucci were used. The obtained material was subjected to statistical analysis using probability distribution, U-test, t-student test, and chi 2 as well as the Statistica 7.1 software package.
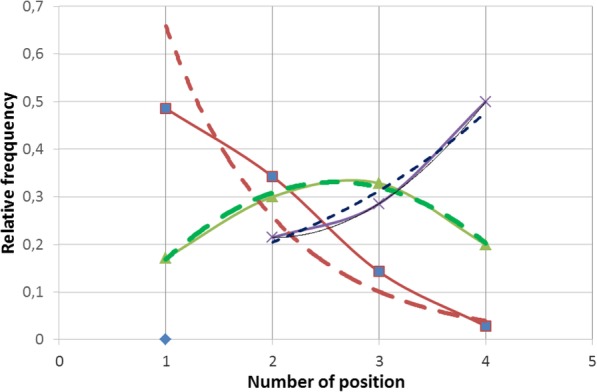
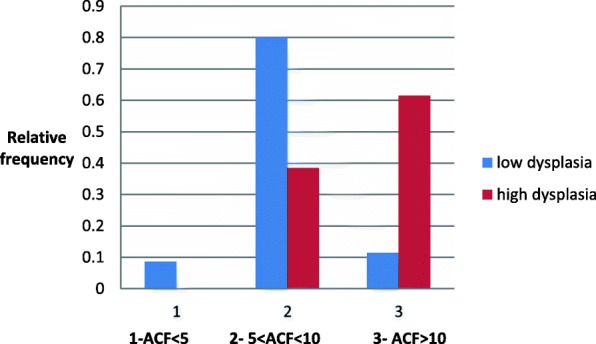
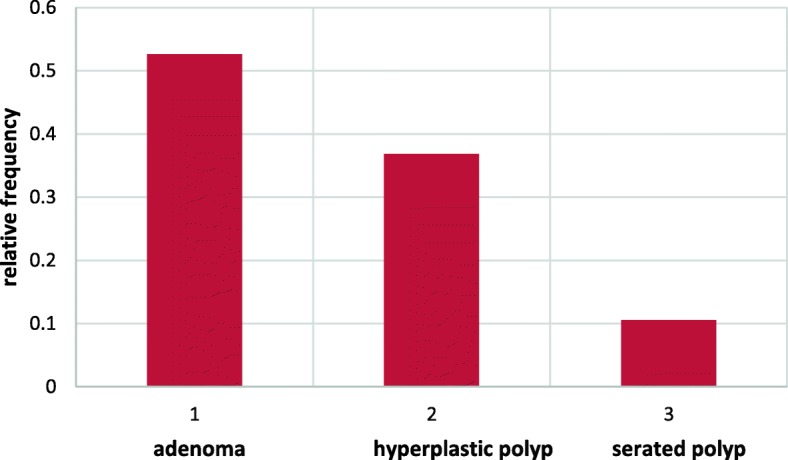
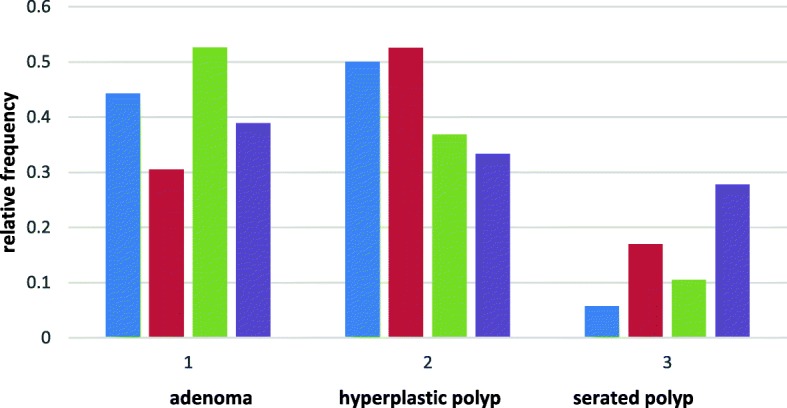
Results: The study population was divided into three subgroups according to the number of ACF observed, i.e. ACF < 5, 5-10 and > 10. ACF < 5 were found in 35 patients (29.41%), 5-10 ACF in 70 (58.82%) and ACF > 10 in 14 individuals (11.76%). The study revealed the presence of normal ACF (p = 0.49), hyperplastic ACF (p = 0.34), dysplastic ACF (p = 0.11), and mixed ACF (p = 0.06). A single type of ACF was most commonly observed (n = 88, p = 0.74). In the researched group a larger number of ACF is concurrent with adenomas and hyperplastic polyps. The number of ACF clearly correlates with the dysplasia advancement in the adenoma and the number of polyps found.
Conclusions: Rectal ACF are a useful marker for the presence of cancerous lesions in the proximal and distal sections of the large intestine.
Keywords: Benign and malignant neoplastic lesions; Large intestine; Rectal ACF.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
