

The risk of morbidity and mortality following recurrent malaria in Papua, Indonesia: a retrospective cohort study
- PMID: 32075649
- PMCID: PMC7031957
- DOI: 10.1186/s12916-020-1497-0
The risk of morbidity and mortality following recurrent malaria in Papua, Indonesia: a retrospective cohort study
Abstract
Background: An acute episode of malaria can be followed by multiple recurrent episodes either due to re-infection, recrudescence of a partially treated parasite or, in the case of Plasmodium vivax or P. ovale, relapse from the dormant liver stage of the parasite. The aim of this study was to quantify the impact of recurrent malaria episodes on morbidity and mortality in Papua, Indonesia.
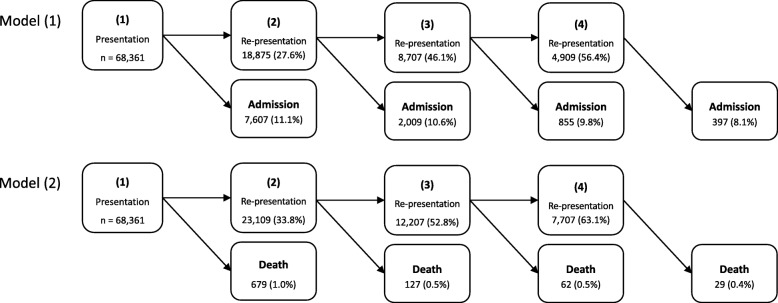
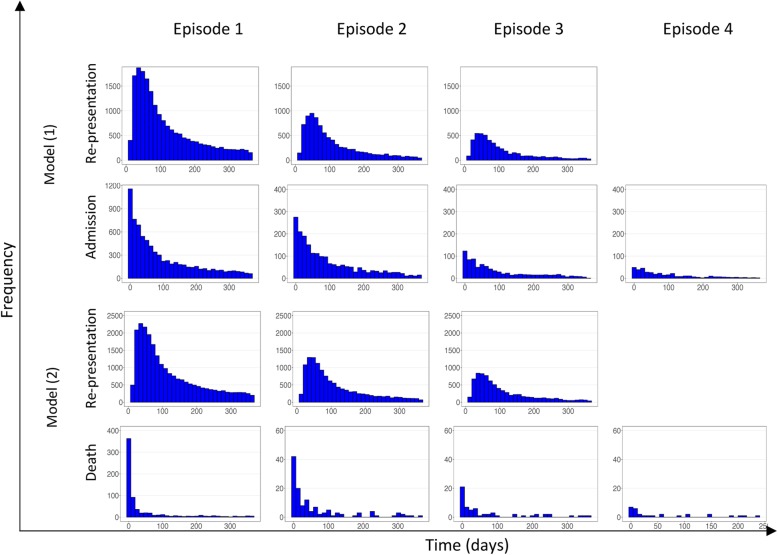
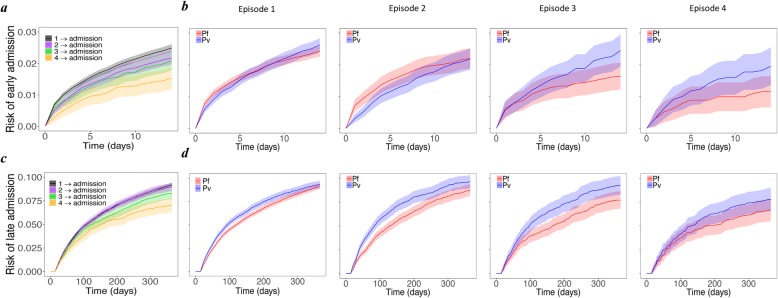
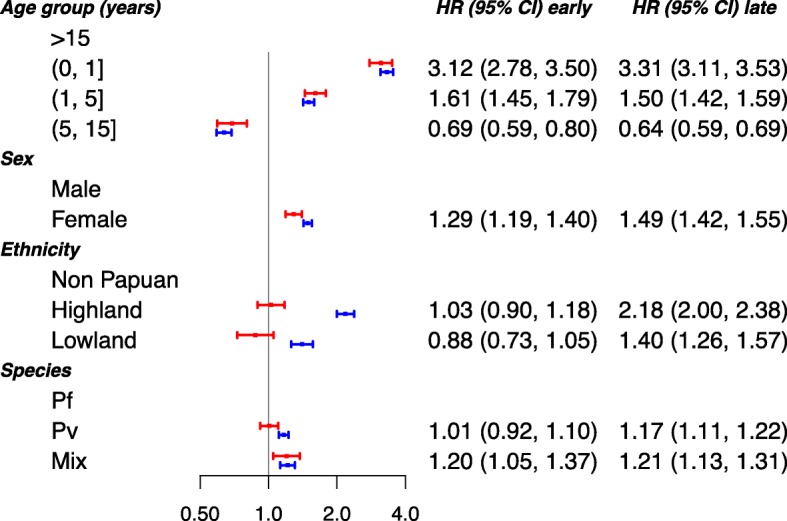
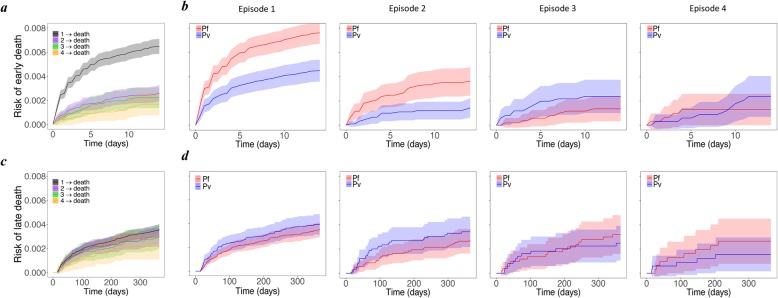
Methods: We undertook a retrospective analysis of routinely collected data from malaria patients attending the primary referral hospital in Papua, Indonesia, between April 2004 and December 2013. Multi-state modelling was used to estimate the effect of recurring malaria episodes on re-presentation and admission to hospital and death. The risks of early (≤ 14 days) and late (15 to 365 days) hospital admission and death were estimated separately in our study to distinguish between the direct and indirect effects of malaria recurrence on adverse outcomes.
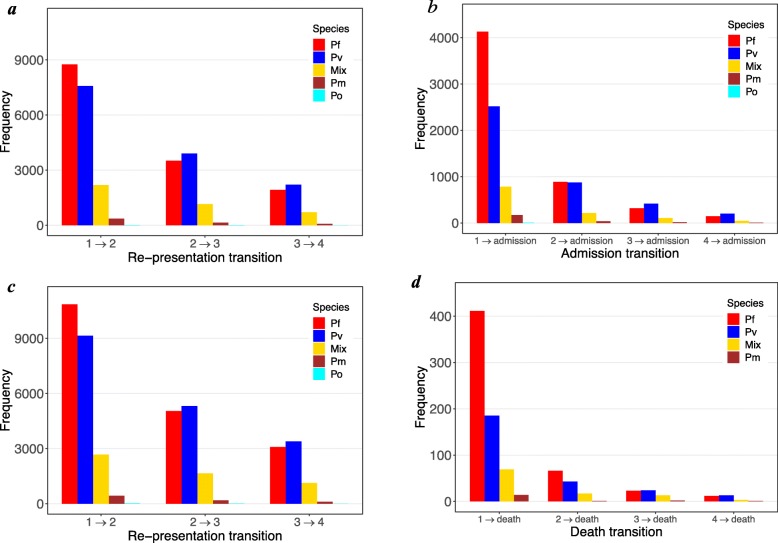
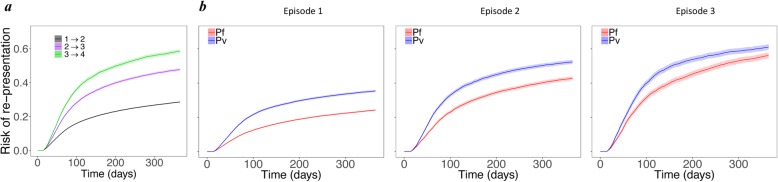
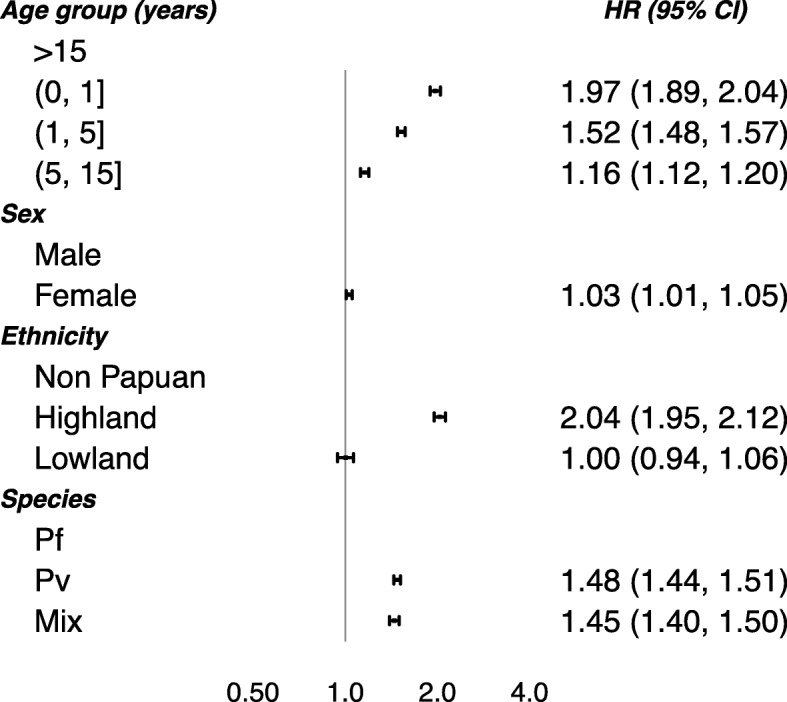
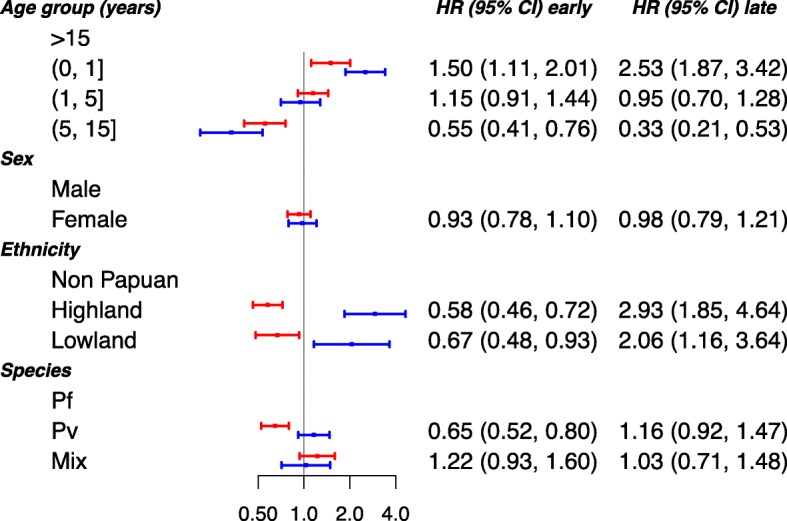
Results: A total of 68,361 patients were included in the analysis, of whom 37,168 (54.4%) presented initially with P. falciparum, 22,209 (32.5%) with P. vivax, and 8984 (13.1%) with other species. During 12 months of follow-up after each of the first four malaria episodes, 10,868 (15.9%) patients were admitted to hospital and 897 (1.3%) died. The risk of re-presenting to the hospital with malaria increased from 34.7% (95% CI 34.4%, 35.1%) at first episode to 58.6% (57.5%, 59.6%) following the third episode of malaria. After adjusting for co-factors, infection with P. vivax was a significant risk factor for re-presentation (hazard ratio (HR) = 1.48 (95% CI 1.44, 1.51)) and late admission to hospital (HR = 1.17 (1.11, 1.22)). Patients infected with P. falciparum had a greater overall rate of mortality within 14 days (HR = 1.54 (1.25, 1.92)), but after multiple episodes of malaria, there was a trend towards a higher rate of early death in patients infected with P. vivax compared to P. falciparum (HR = 1.91 (0.73, 4.97)).
Conclusions: Compared to patients initially infected with P. falciparum, those infected with P. vivax had significantly more re-presentations to hospital with malaria, and this contributed to a high risk of inpatient admission and death. These findings highlight the importance of radical cure of P. vivax to eliminate the dormant liver stages that trigger relapses.
Keywords: Falciparum; Indonesia; Malaria recurrence; Papua; Plasmodium; Vivax.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization (WHO) World Malaria Report 2018. Geneva: World Health Organisation; 2016.
-
- Devine A, Parmiter M, Chu CS, Bancone G, Nosten F, Price RN, et al. Using G6PD tests to enable the safe treatment of Plasmodium vivax infections with primaquine on the Thailand-Myanmar border: a cost-effectiveness analysis. PLoS Negl Trop Dis. 2017;11:e0005602. doi: 10.1371/journal.pntd.0005602. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
