

Trends and risk factors of mortality and disability adjusted life years for chronic respiratory diseases from 1990 to 2017: systematic analysis for the Global Burden of Disease Study 2017
- PMID: 32075787
- PMCID: PMC7190065
- DOI: 10.1136/bmj.m234
Trends and risk factors of mortality and disability adjusted life years for chronic respiratory diseases from 1990 to 2017: systematic analysis for the Global Burden of Disease Study 2017
Erratum in
-
Trends and risk factors of mortality and disability adjusted life years for chronic respiratory diseases from 1990 to 2017: systematic analysis for the Global Burden of Disease Study 2017.BMJ. 2020 Aug 6;370:m3150. doi: 10.1136/bmj.m3150. BMJ. 2020. PMID: 32763968 Free PMC article. No abstract available.
Abstract
Objective: To describe the temporal and spatial trends of mortality and disability adjusted life years (DALYs) due to chronic respiratory diseases, by age and sex, across the world during 1990-2017 using data from the Global Burden of Disease Study 2017.
Design: Systematic analysis.
Data source: The Global Burden of Diseases, Injuries, and Risk Factors Study 2017.
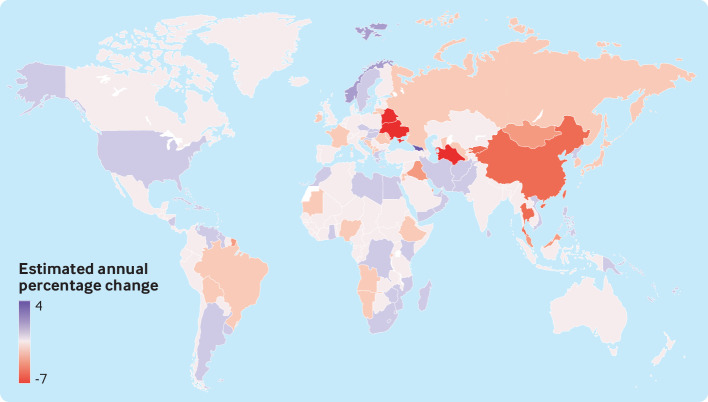
Methods: Mortality and DALYs from chronic respiratory diseases were estimated from the Global Burden of Disease Study 2017 using DisMod-MR 2.1, a Bayesian meta-regression tool. The estimated annual percentage change of the age standardised mortality rate was calculated using a generalised linear model with a Gaussian distribution. Mortality and DALYs were stratified according to the Socio-demographic index. The strength and direction of the association between the Socio-demographic index and mortality rate were measured using the Spearman rank order correlation. Risk factors for chronic respiratory diseases were analysed from exposure data.
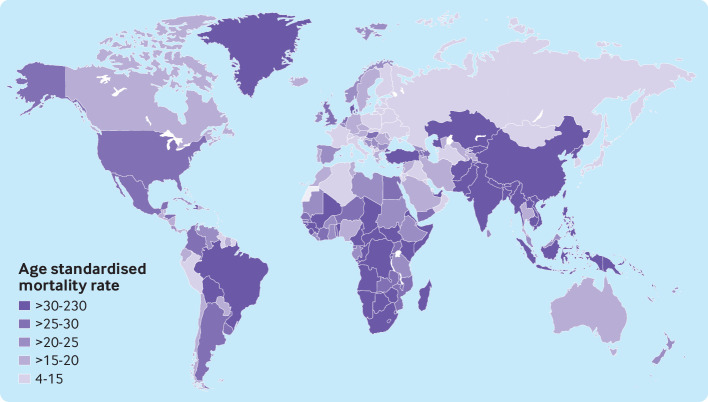
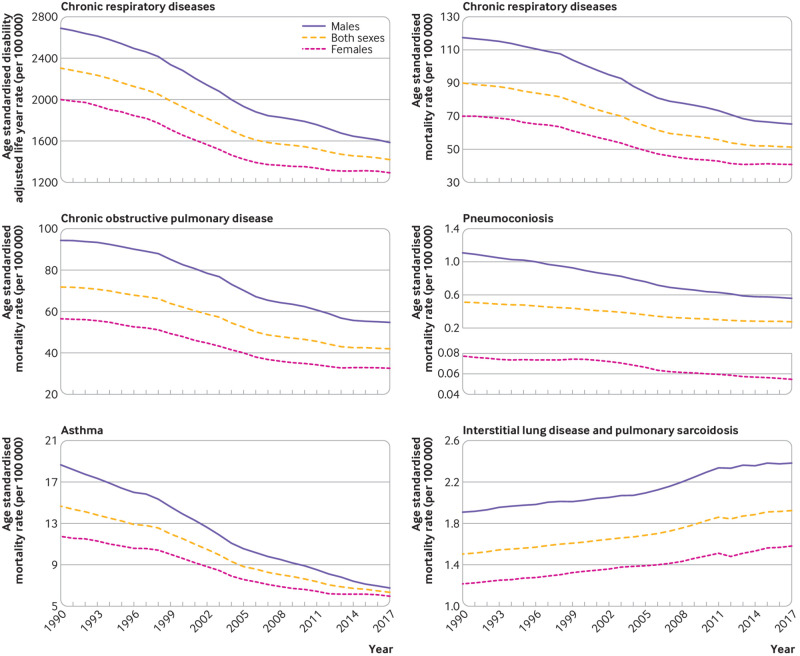
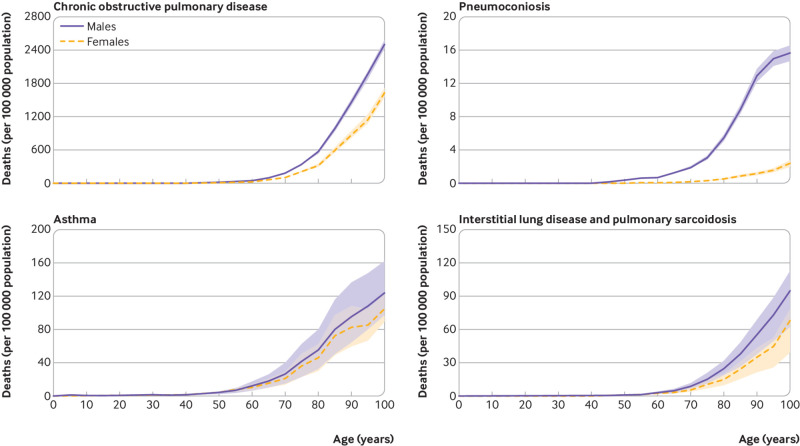
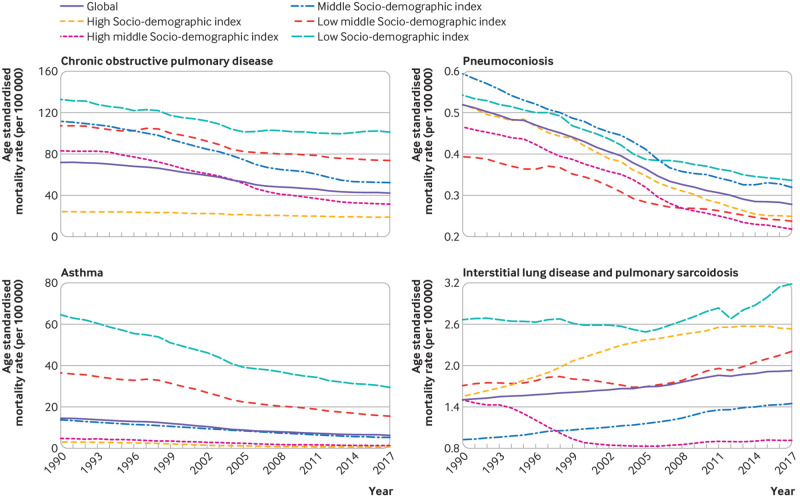
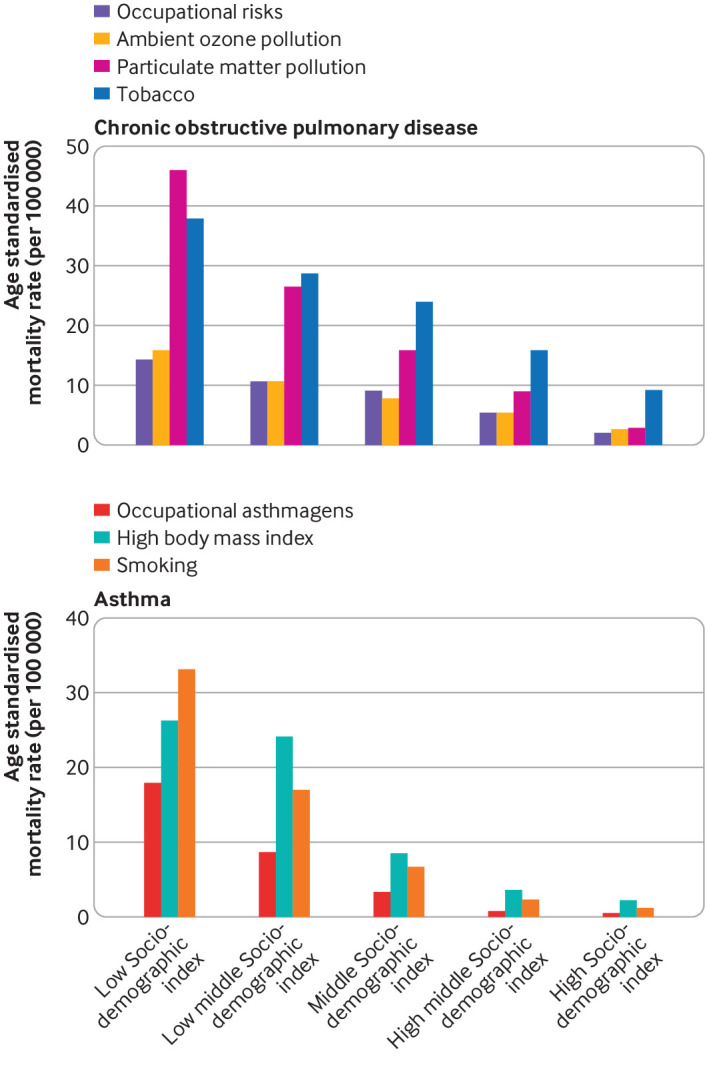
Results: Between 1990 and 2017, the total number of deaths due to chronic respiratorydiseases increased by 18.0%, from 3.32 (95% uncertainty interval 3.01 to 3.43) million in 1990 to 3.91 (3.79 to 4.04) million in 2017. The age standardised mortality rate of chronic respiratory diseases decreased by an average of 2.41% (2.28% to 2.55%) annually. During the 27 years, the annual decline in mortality rates of chronic obstructive pulmonary disease (COPD; 2.36%, uncertainty interval 2.21% to 2.50%) and pneumoconiosis (2.56%, 2.44% to 2.68%) has been slow, whereas the mortality rate for interstitial lung disease and pulmonary sarcoidosis (0.97%, 0.92% to 1.03%) has increased. Reductions in DALYs for asthma and pneumoconiosis have been seen, but DALYs due to COPD, and interstitial lung disease and pulmonary sarcoidosis have increased. Mortality and the annual change in mortality rate due to chronic respiratory diseases varied considerably across 195 countries. Assessment of the factors responsible for regional variations in mortality and DALYs and the unequal distribution of improvements during the 27 years showed negative correlations between the Socio-demographic index and the mortality rates of COPD, pneumoconiosis, and asthma. Regions with a low Socio-demographic index had the highest mortality and DALYs. Smoking remained the major risk factor for mortality due to COPD and asthma. Pollution from particulate matter was the major contributor to deaths from COPD in regions with a low Socio-demographic index. Since 2013, a high body mass index has become the principal risk factor for asthma.
Conclusions: Regions with a low Socio-demographic index had the greatest burden of disease. The estimated contribution of risk factors (such as smoking, environmental pollution, and a high body mass index) to mortality and DALYs supports the need for urgent efforts to reduce exposure to them.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the National Key R&D Program of China and the National Natural Science Foundation of China for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical