

A geometrically adaptable heart valve replacement
- PMID: 32075944
- PMCID: PMC7425635
- DOI: 10.1126/scitranslmed.aay4006
A geometrically adaptable heart valve replacement
Abstract
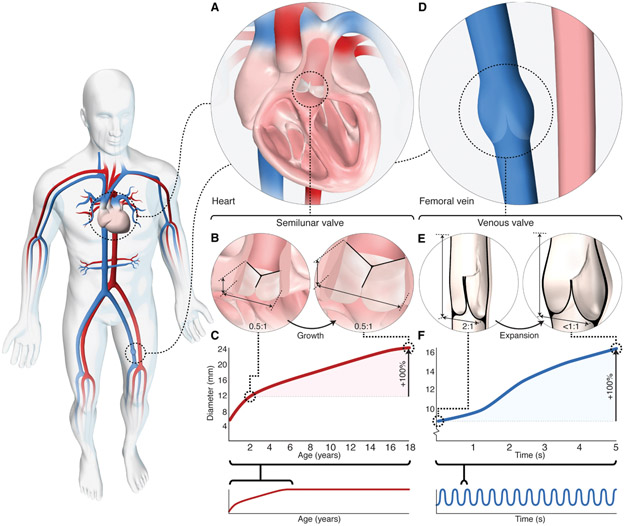
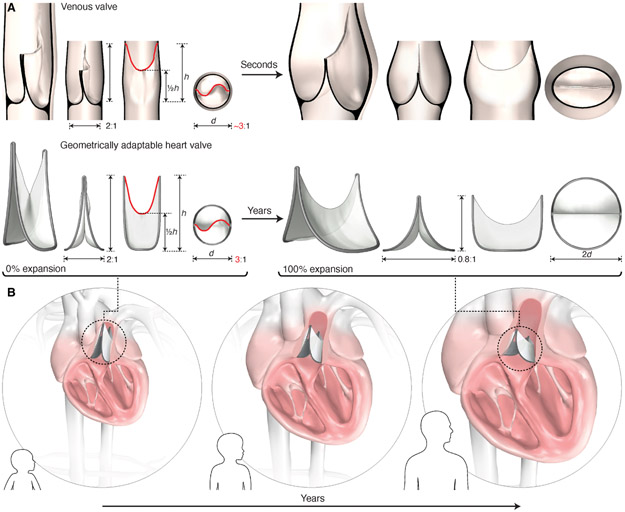
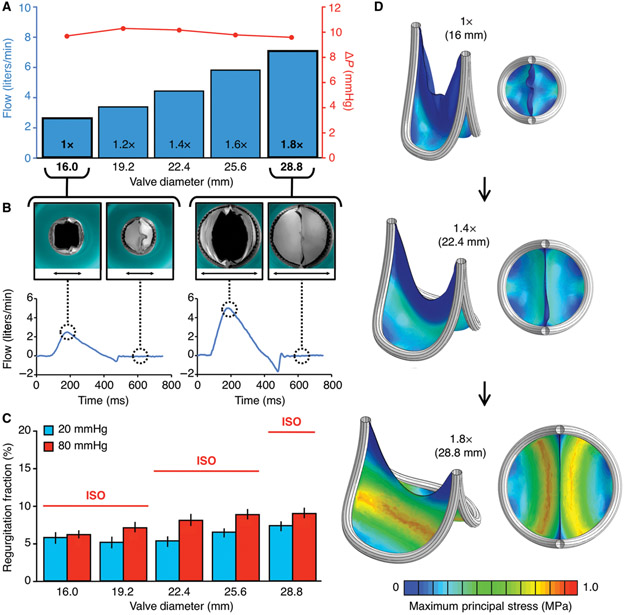
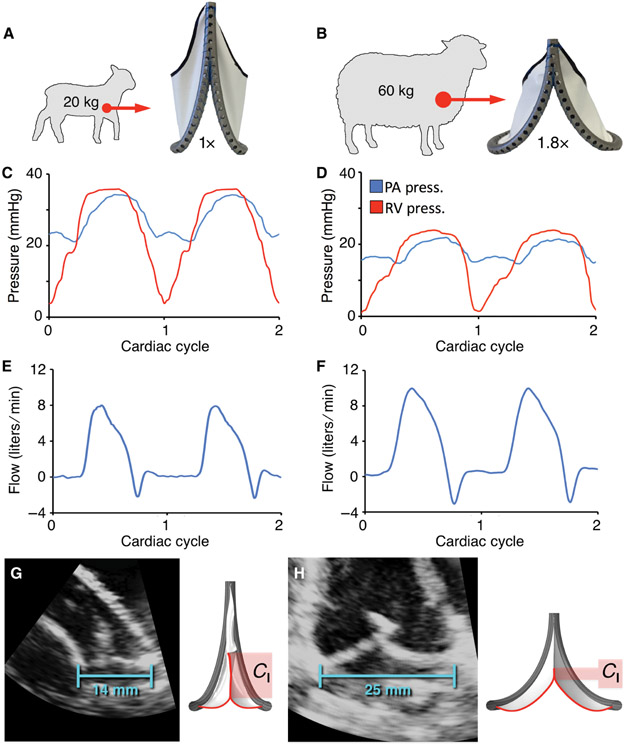
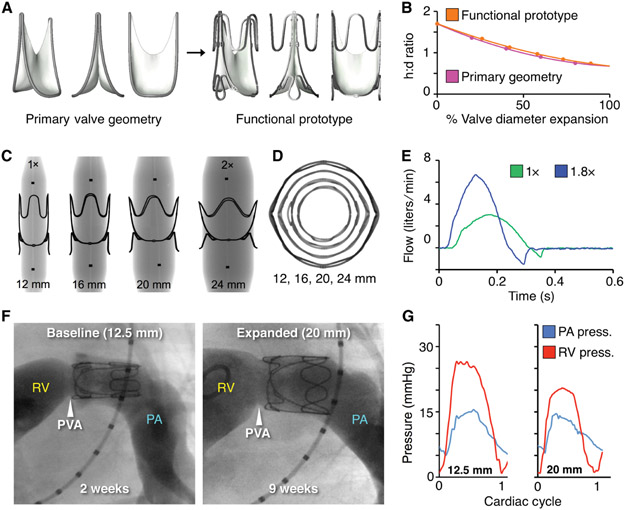
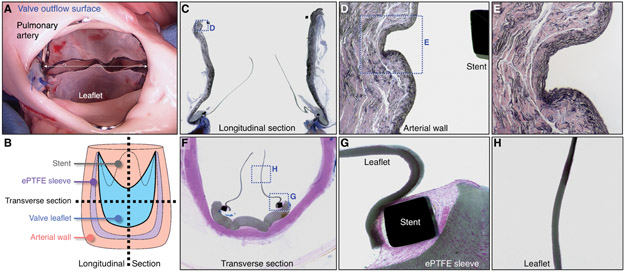
Congenital heart valve disease has life-threatening consequences that warrant early valve replacement; however, the development of a growth-accommodating prosthetic valve has remained elusive. Thousands of children continue to face multiple high-risk open-heart operations to replace valves that they have outgrown. Here, we demonstrate a biomimetic prosthetic valve that is geometrically adaptable to accommodate somatic growth and structural asymmetries within the heart. Inspired by the human venous valve, whose geometry is optimized to preserve functionality across a wide range of constantly varying volume loads and diameters, our balloon-expandable synthetic bileaflet valve analog exhibits similar adaptability to dimensional and shape changes. Benchtop and acute in vivo experiments validated design functionality, and in vivo survival studies in growing sheep demonstrated that mechanical valve expansion accommodated growth. As illustrated in this work, dynamic size adaptability with preservation of unidirectional flow in prosthetic valves thus offers a paradigm shift in the treatment of heart valve disease.
Copyright © 2020 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Figures
References
-
- van der Linde D, Konings EE, Slager MA, Witsenburg M, Helbing WA, Takkenberg JJ, Roos-Hesselink JW, Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol 58, 2241–2247 (2011). - PubMed
-
- Bernier PL, Stefanescu A, Samoukovic G, Tchervenkov CI, The challenge of congenital heart disease worldwide: epidemiologic and demographic facts. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu 13, 26–34 (2010). - PubMed
-
- Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jimenez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozaffarian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritchey M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P, American C Heart Association Statistics, S. Stroke Statistics, Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation 135, e146–e603 (2017). - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
