Automated Quantitative Extraction and Analysis of 4D flow Patterns in the Ascending Aorta: An intraindividual comparison at 1.5 T and 3 T
- PMID: 32076060
- PMCID: PMC7031260
- DOI: 10.1038/s41598-020-59826-2
Automated Quantitative Extraction and Analysis of 4D flow Patterns in the Ascending Aorta: An intraindividual comparison at 1.5 T and 3 T
Abstract
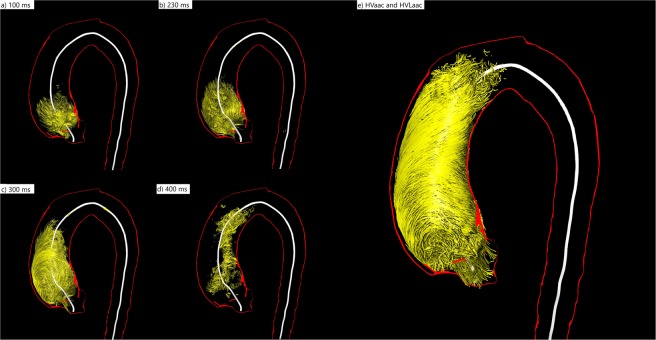
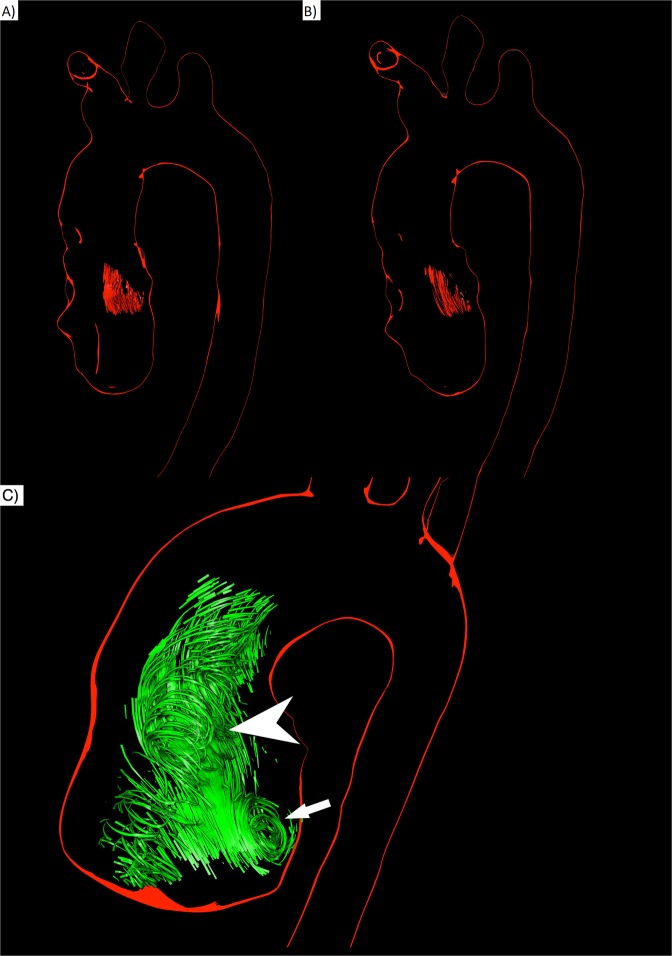
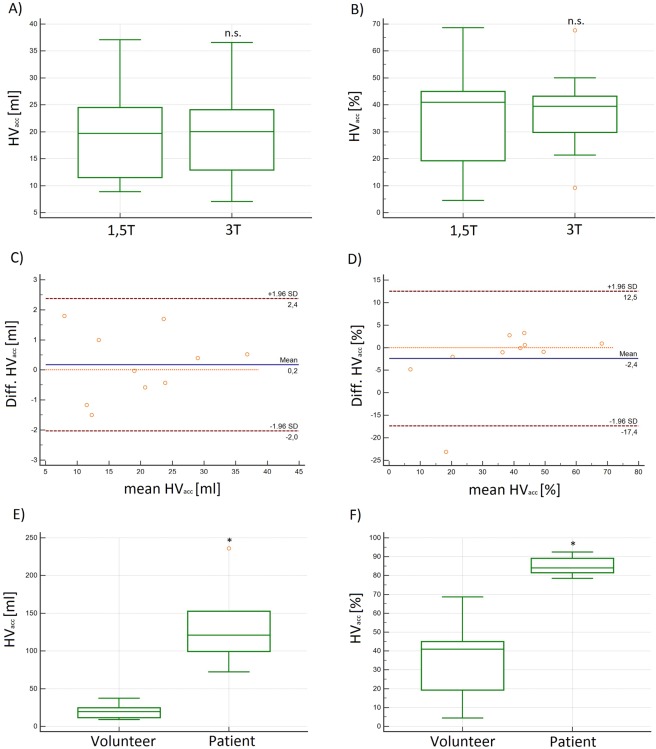
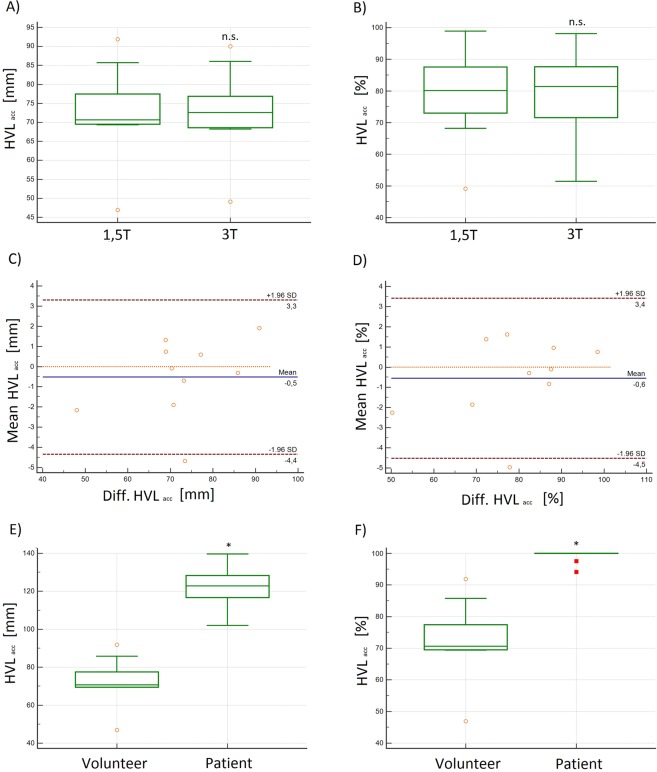
4D flow MRI enables quantitative assessment of helical flow. Current methods are susceptible to noise. To evaluate helical flow patterns in healthy volunteers and patients with bicuspid aortic valves (BAV) at 1.5 T and 3 T using pressure-based helix-extraction in 4D flow MRI. Two intraindividual 4D flow MRI examinations were performed at 1.5 T and 3 T in ten healthy volunteers (5 females, 32 ± 3 years) and 2 patients with BAV using different acceleration techniques (kt-GRAPPA and centra). Several new quantitative parameters for the evaluation of volumes [ml], lengths [mm] as well as temporal parameters [ms] of helical flow were introduced and analyzed using the software tool Bloodline. We found good correlations between measurements in volunteers at 1.5 T and 3 T regarding helical flow volumes (R = 0.98) and temporal existence (R = 0.99) of helices in the ascending aorta. Furthermore, we found significantly larger (11.7 vs. 77.6 ml) and longer lasting (317 vs. 769 ms) helices in patients with BAV than in volunteers. The assessed parameters do not depend on the magnetic field strength used for the acquisition. The technique of pressure-based extraction of 4D flow MRI pattern is suitable for differentiation of normal and pathological flow.
Conflict of interest statement
The authors declare no competing interests.
Figures