

Outcome of older (≥70 years) APL patients frontline treated with or without arsenic trioxide-an International Collaborative Study
- PMID: 32076120
- PMCID: PMC8318880
- DOI: 10.1038/s41375-020-0758-4
Outcome of older (≥70 years) APL patients frontline treated with or without arsenic trioxide-an International Collaborative Study
Erratum in
-
Publisher Correction: Outcome of older (≥70 years) APL patients frontline treated with or without arsenic trioxide-an International Collaborative Study.Leukemia. 2021 Dec;35(12):3631. doi: 10.1038/s41375-021-01358-3. Leukemia. 2021. PMID: 34785795 Free PMC article. No abstract available.
Abstract
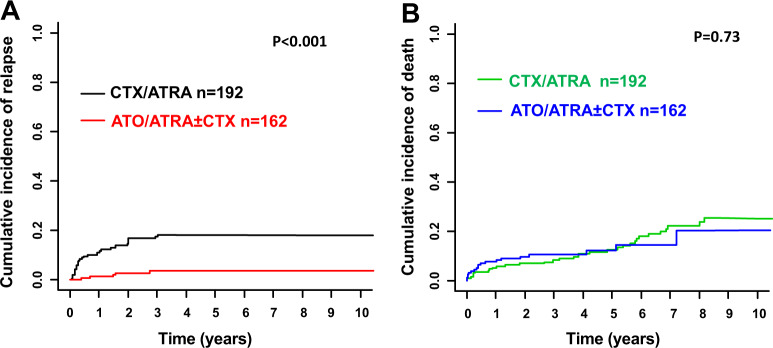
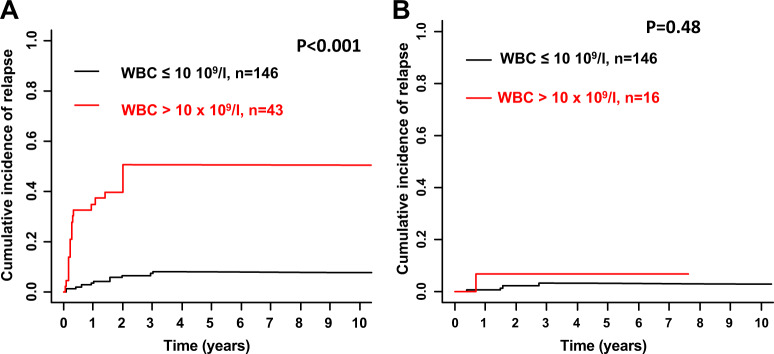
Data on outcome in older (≥70 years) patients with acute promyelocytic leukemia after treatment with arsenic trioxide (ATO) compared with standard chemotherapy (CTX) is scarce. We evaluated 433 patients (median age, 73.4 years) treated either with ATO+ all-trans retinoic acid (ATO/ATRA; n = 26), CTX/ATRA + ATO during consolidation (CTX/ATRA/ATO; n = 148), or with CTX/ATRA (n = 259). Median follow-up for overall survival (OS) was 4.8 years. Complete remissions (CR) were achieved in 92% with ATO/ATRA and 82% with CTX/ATRA; induction death rates were 8% and 18%, respectively. For analysis of postremission outcomes we combined the ATO/ATRA and CTX/ATRA/ATO groups (ATO/ATRA ± CTX). Cumulative incidence of relapse (CIR) was significantly lower after ATO/ATRA ± CTX compared with CTX/ATRA (P < 0.001). The same held true when restricting the analysis according to the treatment period after the year 2000. OS of patients in CR1 was not different between ATO/ATRA ± CTX compared with CTX/ATRA (P = 0.20). High (>10 × 109/l) white blood cell (WBC) counts at diagnosis were associated with higher CIR (P < 0.001) compared with lower WBC in the CTX/ATRA group, but not in the ATO/ATRA ± CTX group (P = 0.48). ATO, when added to ATRA or CTX/ATRA is feasible and effective in elderly patients for remission induction and consolidation, particularly in patients with high WBC at diagnosis.
Conflict of interest statement
SK was supported by the Olympia-Morata fellowship program from the Medical Faculty of the Heidelberg University. MJL is supported by a grant from the NCI (NCI Leukemia SPORE P50 CA100632). UP has received research support from TEVA. All other authors declare no competing conflict of interest.
Figures

References
-
- Lo-Coco F, Avvisati G, Vignetti M, et al. Retinoic acid and arsenic trioxide for acute promyelocytic leukemia. N Engl J Med. 2013;369:111–21. - PubMed
-
- Platzbecker U, Avvisati G, Cicconi L, et al. Improved outcomes with retinoic acid and arsenic trioxide compared with retinoic acid and chemotherapy in non-high-risk acute promyelocytic leukemia: final results of the randomized Italian-German APL0406 trial. J Clin Oncol. 2016;35:605–12. - PubMed
-
- Testa U, Lo-Coco F. Prognostic factors in acute promyelocytic leukemia: strategies to define high-risk patients. Ann Hematol. 2016;95:673–80. - PubMed
-
- Sanz MA, Lo Coco F, Martín G, et al. Definition of relapse risk and role of nonanthracycline drugs for consolidation in patients with acute promyelocytic leukemia: a joint study of the PETHEMA and GIMEMA cooperative groups. Blood. 2000;96:1247–53. - PubMed
-
- Sanz MA, Martin G, Gonzalez M, et al. Risk-adapted treatment of acute promyelocytic leukemia with alltrans-retinoic acid and anthracycline monochemotherapy: a multicenter study by the PETHEMA group. Blood. 2004;103:1237–43. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
