

Improving Accuracy and Efficiency with Concurrent Use of Artificial Intelligence for Digital Breast Tomosynthesis
- PMID: 32076660
- PMCID: PMC6677281
- DOI: 10.1148/ryai.2019180096
Improving Accuracy and Efficiency with Concurrent Use of Artificial Intelligence for Digital Breast Tomosynthesis
Abstract
Purpose: To evaluate the use of artificial intelligence (AI) to shorten digital breast tomosynthesis (DBT) reading time while maintaining or improving accuracy.
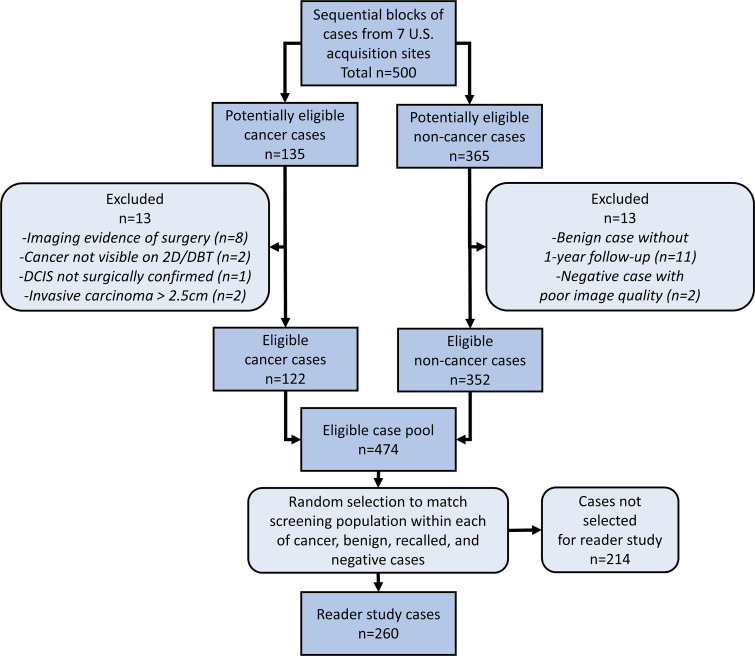
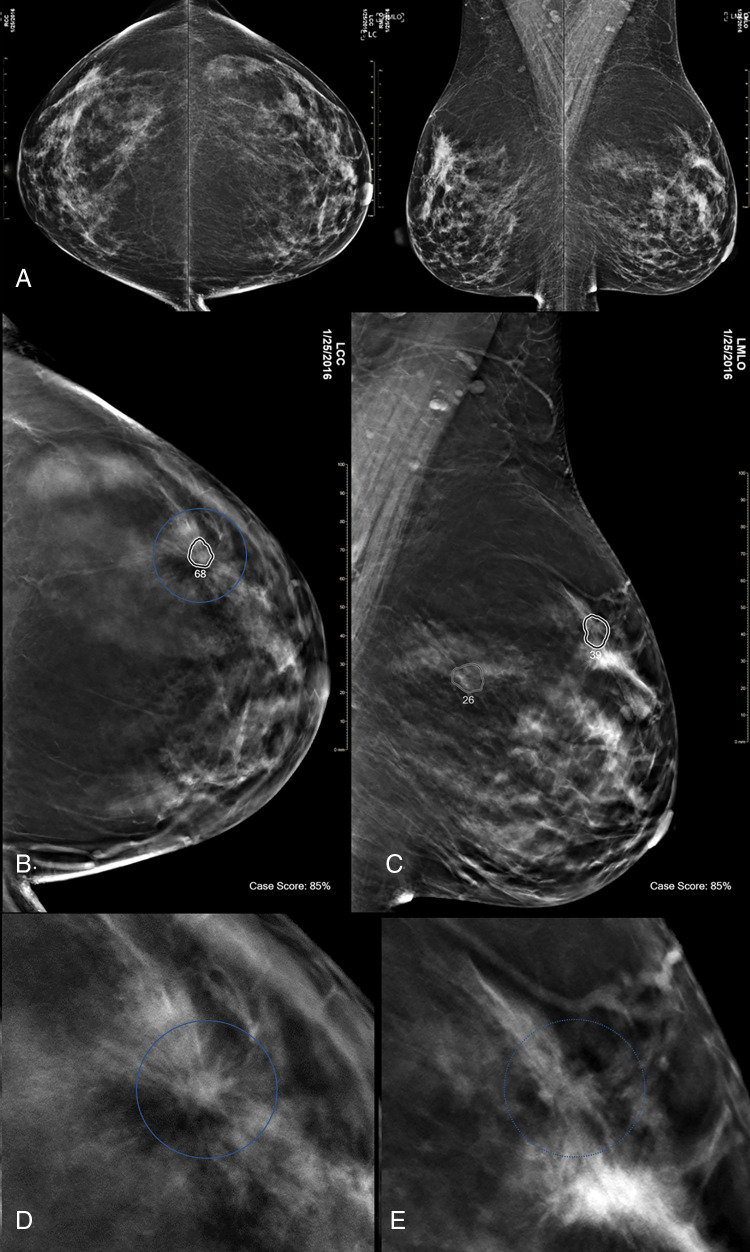
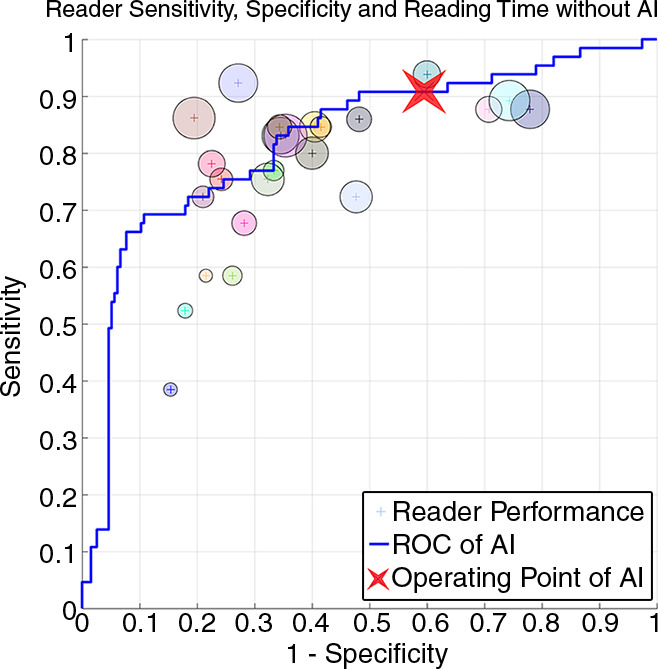
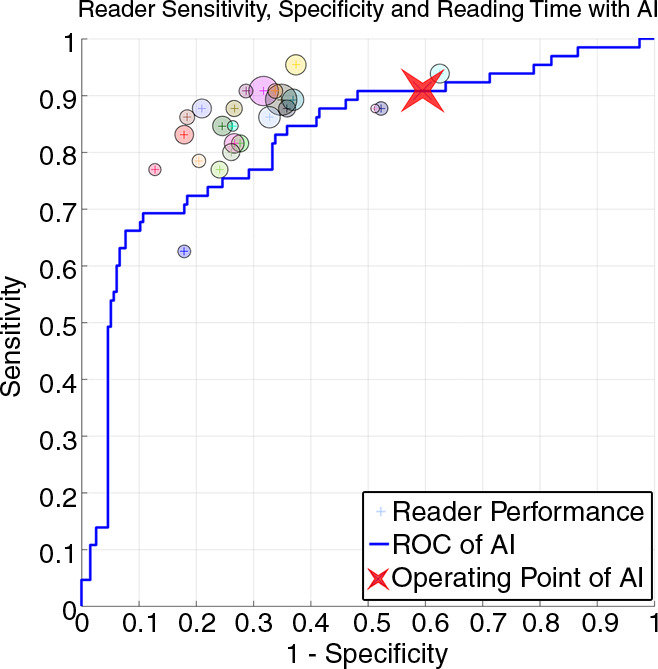
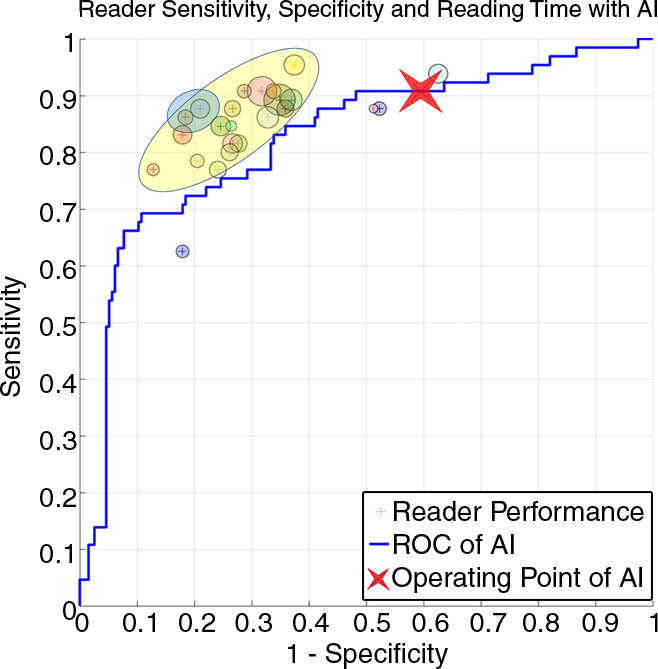
Materials and methods: A deep learning AI system was developed to identify suspicious soft-tissue and calcified lesions in DBT images. A reader study compared the performance of 24 radiologists (13 of whom were breast subspecialists) reading 260 DBT examinations (including 65 cancer cases) both with and without AI. Readings occurred in two sessions separated by at least 4 weeks. Area under the receiver operating characteristic curve (AUC), reading time, sensitivity, specificity, and recall rate were evaluated with statistical methods for multireader, multicase studies.
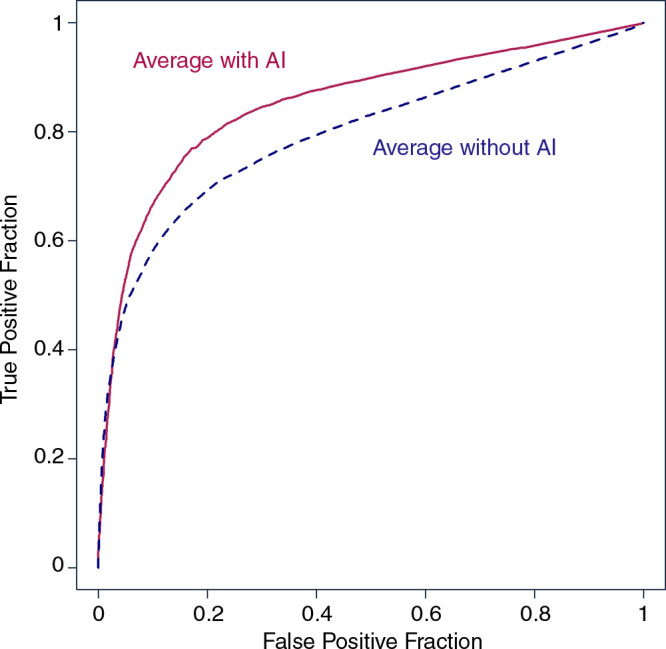
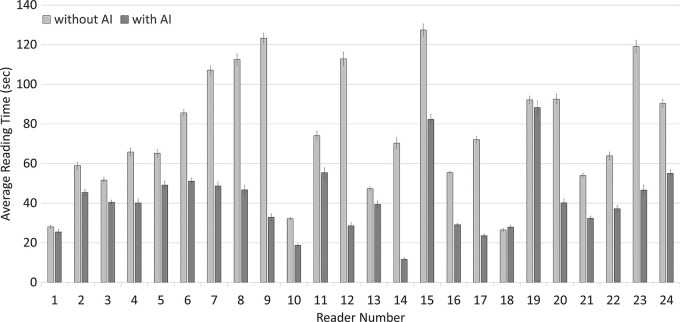
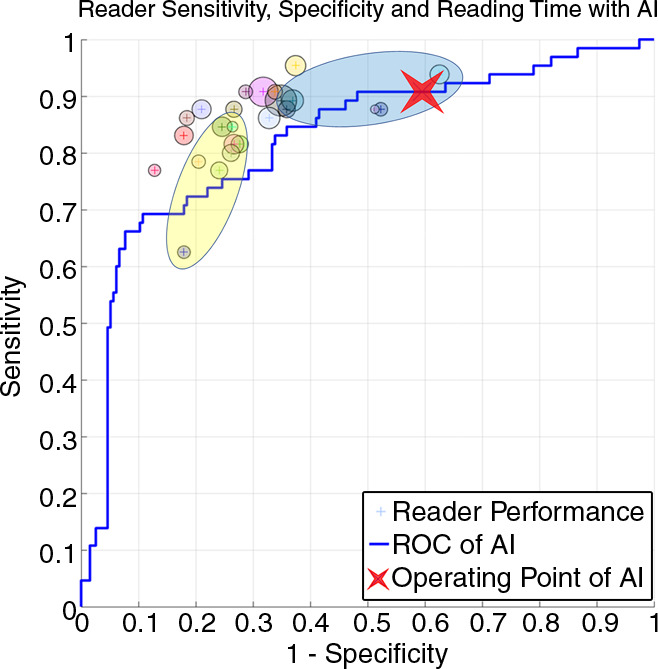
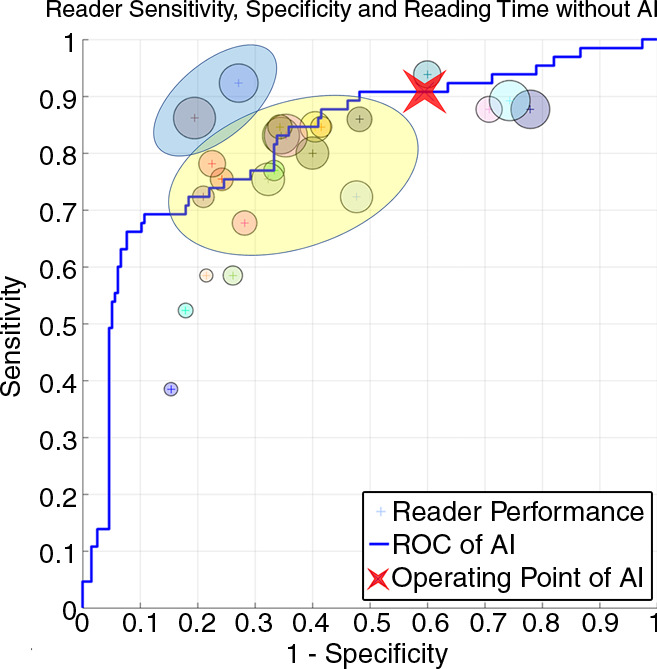
Results: Radiologist performance for the detection of malignant lesions, measured by mean AUC, increased 0.057 with the use of AI (95% confidence interval [CI]: 0.028, 0.087; P < .01), from 0.795 without AI to 0.852 with AI. Reading time decreased 52.7% (95% CI: 41.8%, 61.5%; P < .01), from 64.1 seconds without to 30.4 seconds with AI. Sensitivity increased from 77.0% without AI to 85.0% with AI (8.0%; 95% CI: 2.6%, 13.4%; P < .01), specificity increased from 62.7% without to 69.6% with AI (6.9%; 95% CI: 3.0%, 10.8%; noninferiority P < .01), and recall rate for noncancers decreased from 38.0% without to 30.9% with AI (7.2%; 95% CI: 3.1%, 11.2%; noninferiority P < .01).
Conclusion: The concurrent use of an accurate DBT AI system was found to improve cancer detection efficacy in a reader study that demonstrated increases in AUC, sensitivity, and specificity and a reduction in recall rate and reading time.© RSNA, 2019See also the commentary by Hsu and Hoyt in this issue.
2019 by the Radiological Society of North America, Inc.
Conflict of interest statement
Figures


Comment in
-
Using Time as a Measure of Impact for AI Systems: Implications in Breast Screening.Radiol Artif Intell. 2019 Jul 31;1(4):e190107. doi: 10.1148/ryai.2019190107. eCollection 2019 Jul. Radiol Artif Intell. 2019. PMID: 33937798 Free PMC article. No abstract available.
References
-
- Skaane P, Bandos AI, Gullien R, et al. Comparison of digital mammography alone and digital mammography plus tomosynthesis in a population-based screening program. Radiology 2013;267(1):47–56. - PubMed
-
- Friedewald SM, Rafferty EA, Rose SL, et al. Breast cancer screening using tomosynthesis in combination with digital mammography. JAMA 2014;311(24):2499–2507. - PubMed
-
- Hooley RJ, Durand MA, Philpotts LE. Advances in digital breast tomosynthesis. AJR Am J Roentgenol 2017;208(2):256–266. - PubMed
-
- ACR Statement on Breast Tomosynthesis. American College of Radiology Web site. https://www.acr.org/Advocacy-and-Economics/ACR-Position-Statements/Breas.... Published November 24, 2014. Accessed October 24, 2018.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
