

Cytomegalovirus (CMV) Cell-Mediated Immunity and CMV Infection After Allogeneic Hematopoietic Cell Transplantation: The REACT Study
- PMID: 32076709
- PMCID: PMC7713694
- DOI: 10.1093/cid/ciz1210
Cytomegalovirus (CMV) Cell-Mediated Immunity and CMV Infection After Allogeneic Hematopoietic Cell Transplantation: The REACT Study
Abstract
Background: Cytomegalovirus (CMV) infection remains an important cause of morbidity and mortality in allogeneic hematopoietic cell transplant (allo-HCT) recipients. CMV cell-mediated immunity (CMV-CMI) as determined by a peptide-based enzyme-linked immunospot (ELISPOT) CMV assay may identify patients at risk for clinically significant CMV infection (CS-CMVi).
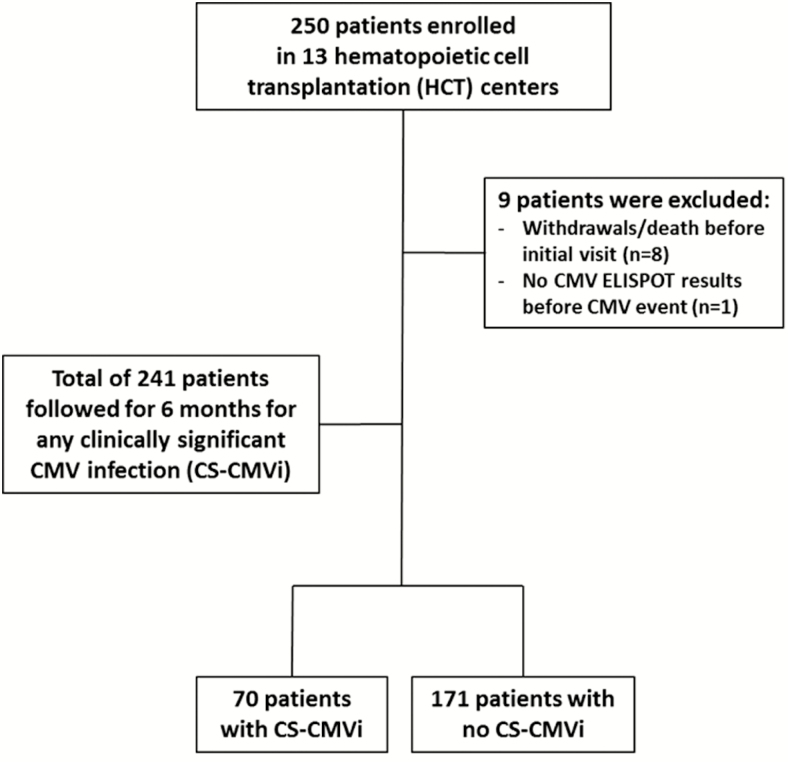
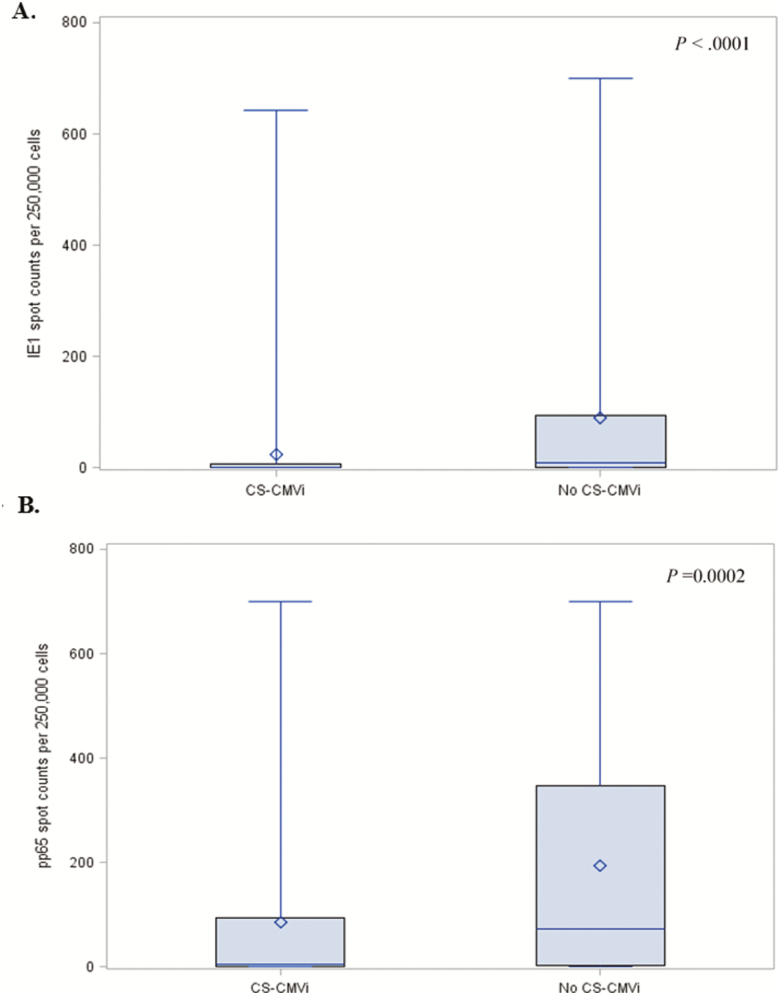
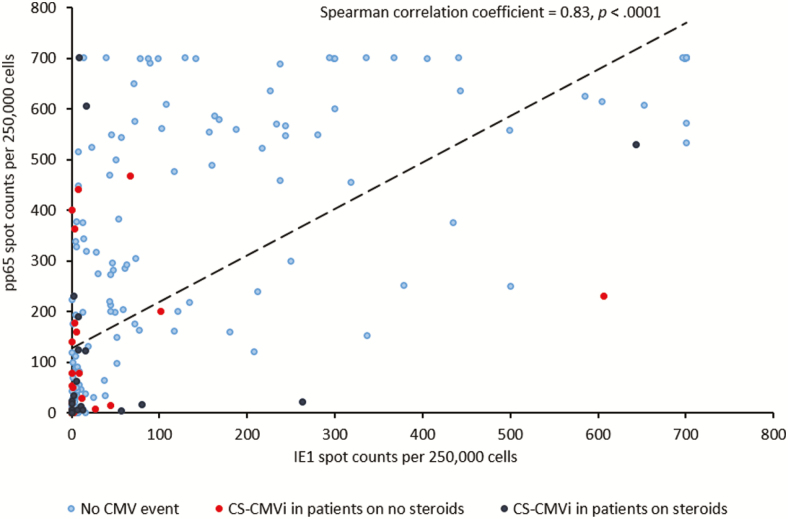
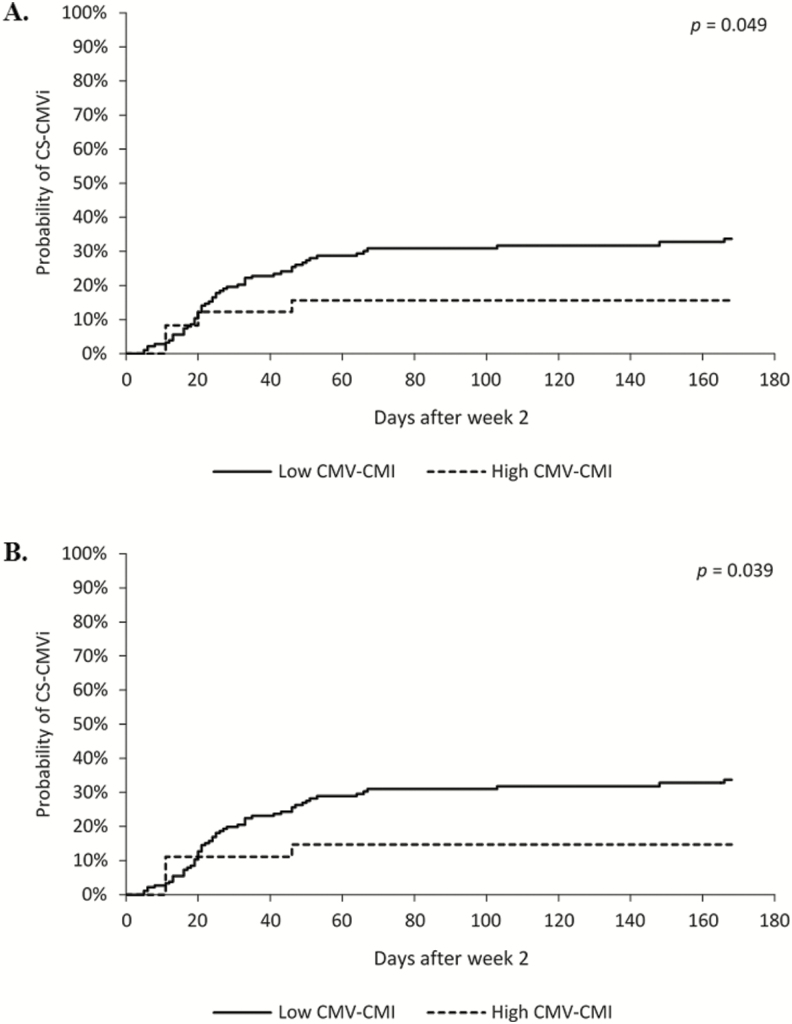
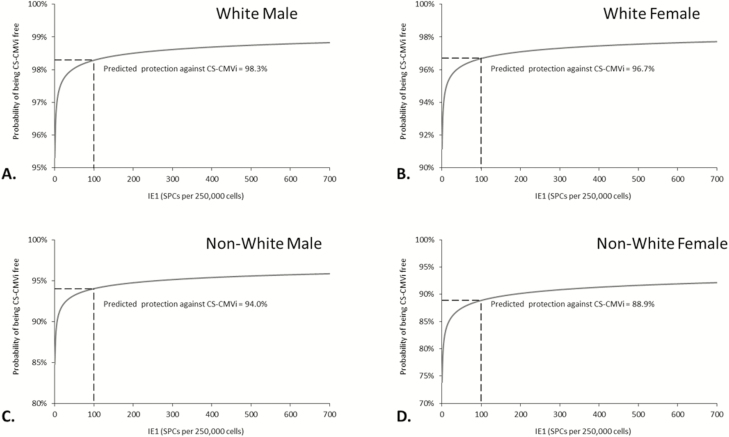
Methods: The CS-CMVi was defined as CMV viremia and/or disease necessitating antiviral therapy. CMV-CMI was characterized as high when the intermediate-early 1 (IE-1) antigen spot counts (SPCs) were >100 (cutoff 1) or when the IE-1 and phosphoprotein 65 antigen SPCs were both >100 SPCs per 250 000 cells (cutoff 2), and a low CMV-CMI when SPCs were below these thresholds. In this prospective multicenter study, we evaluated CMV-CMI every 2 weeks from the pretransplant period until 6 months posttransplantation in 241 allo-HCT recipients with positive CMV serostatus. The primary endpoint was CS-CMVi occurring within 2 weeks of the last measurement of CMV-CMI.
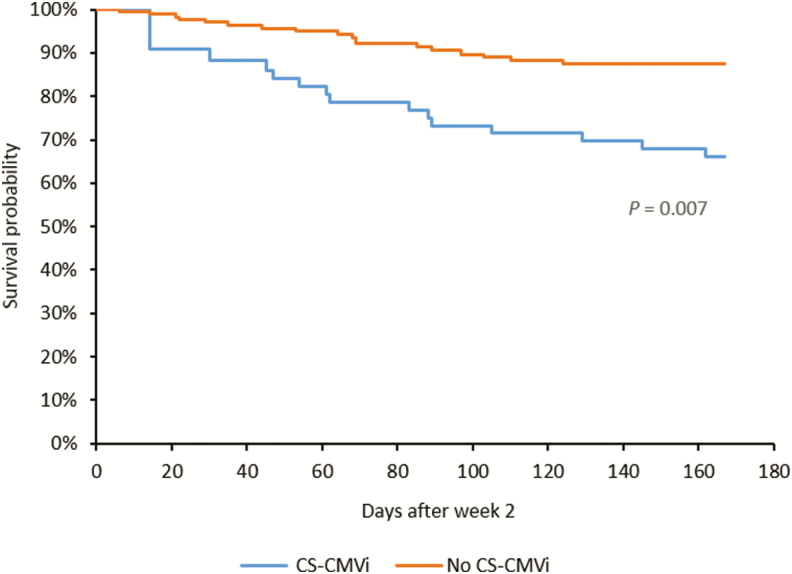
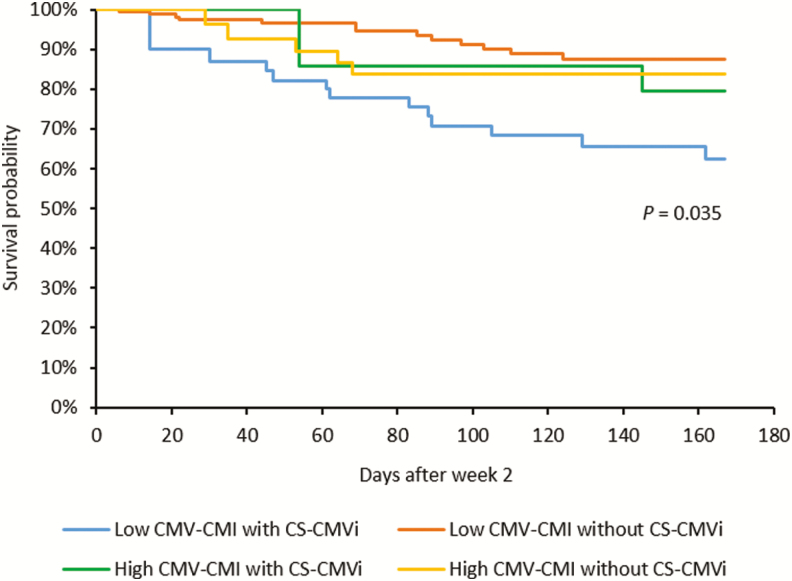
Results: CS-CMVi occurred in 70 allo-HCT recipients (29%). CMV-CMI was low in patients who experienced CS-CMVi (94%), whereas those who had a high CMV-CMI were less likely to have CS-CMVi (P < .0001). Patients with CS-CMVi had higher all-cause mortality (P = .007), especially those with low CMV-CMI (P = .035). On multivariable analysis, CMV-CMI, sex, race, antithymocyte globulin, and steroid use were independent predictors of CS-CMVi, and the time from transplant to engraftment was the only predictor of mortality.
Conclusions: Measurement of CMV-CMI using a novel ELISPOT assay would be useful clinically to monitor allo-HCT recipients and distinguish between those at risk of developing CS-CMVi and requiring antiviral prophylaxis or therapy and those who are protected.
Keywords: CMV ELISPOT assay; cell-mediated immunity; cytomegalovirus; hematopoietic cell transplant; multicenter.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Interferon-γ Release Assay for Cytomegalovirus (IGRA-CMV) for Risk Stratification of Posttransplant CMV Infection: Is It Time to Apply IGRA-CMV in Routine Clinical Practice?Clin Infect Dis. 2020 Dec 3;71(9):2386-2388. doi: 10.1093/cid/ciz1211. Clin Infect Dis. 2020. PMID: 32076699 No abstract available.
References
-
- Nichols WG, Corey L, Gooley T, Davis C, Boeckh M. High risk of death due to bacterial and fungal infection among cytomegalovirus (CMV)-seronegative recipients of stem cell transplants from seropositive donors: evidence for indirect effects of primary CMV infection. J Infect Dis 2002; 185:273–82. - PubMed
-
- Yong MK, Ananda-Rajah M, Cameron PU, et al. Cytomegalovirus reactivation is associated with increased risk of late-onset invasive fungal disease after allogeneic hematopoietic stem cell transplantation: a multicenter study in the current era of viral load monitoring. Biol Blood Marrow Transplant 2017; 23:1961–7. - PubMed
-
- Ariza-Heredia EJ, Nesher L, Chemaly RF. Cytomegalovirus diseases after hematopoietic stem cell transplantation: a mini-review. Cancer Lett 2014; 342:1–8. - PubMed
