

Cancer spectrum and outcomes in the Mendelian short telomere syndromes
- PMID: 32076714
- PMCID: PMC7256360
- DOI: 10.1182/blood.2019003264
Cancer spectrum and outcomes in the Mendelian short telomere syndromes
Abstract
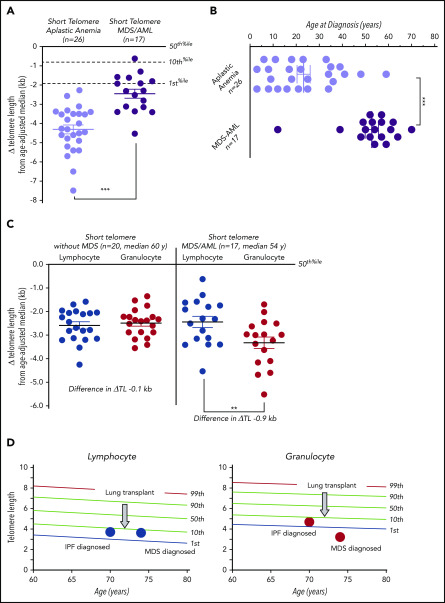
Short telomeres have been linked to cancer risk, yet other evidence supports them being tumor suppressive. Here, we report cancer outcomes in individuals with germline mutations in telomerase and other telomere-maintenance genes. Among 180 individuals evaluated in a hospital-based setting, 12.8% had cancer. Solid tumors were rare (2.8%); nearly all were young male DKC1 mutation carriers, and they were generally resectable with good short-term outcomes. Myelodysplastic syndrome (MDS) was most common, followed by acute myeloid leukemia (AML); they accounted for 75% of cancers. Age over 50 years was the biggest risk factor, and MDS/AML usually manifested with marrow hypoplasia and monosomy 7, but the somatic mutation landscape was indistinct from unselected patients. One- and 2-year survival were 61% and 39%, respectively, and two-thirds of MDS/AML patients died of pulmonary fibrosis and/or hepatopulmonary syndrome. In one-half of the cases, MDS/AML patients showed a recurrent peripheral blood pattern of acquired, granulocyte-specific telomere shortening. This attrition was absent in age-matched mutation carriers who did not have MDS/AML. We tested whether adult short telomere patients without MDS/AML also had evidence of clonal hematopoiesis of indeterminate potential-related mutations and found that 30% were affected. These patients also primarily suffered morbidity from pulmonary fibrosis during follow-up. Our data show that the Mendelian short telomere syndromes are associated with a relatively narrow cancer spectrum, primarily MDS and AML. They suggest that short telomere length is sufficient to drive premature age-related clonal hematopoiesis in these inherited disorders.
© 2020 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures




References
-
- Blasco MA, Lee HW, Hande MP, et al. . Telomere shortening and tumor formation by mouse cells lacking telomerase RNA. Cell. 1997;91(1):25-34. - PubMed
-
- Artandi SE, Chang S, Lee SL, et al. . Telomere dysfunction promotes non-reciprocal translocations and epithelial cancers in mice. Nature. 2000;406(6796):641-645. - PubMed
-
- Hao LY, Armanios M, Strong MA, et al. . Short telomeres, even in the presence of telomerase, limit tissue renewal capacity. Cell. 2005;123(6):1121-1131. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
