

ICU-acquired weakness
- PMID: 32076765
- PMCID: PMC7224132
- DOI: 10.1007/s00134-020-05944-4
ICU-acquired weakness
Abstract
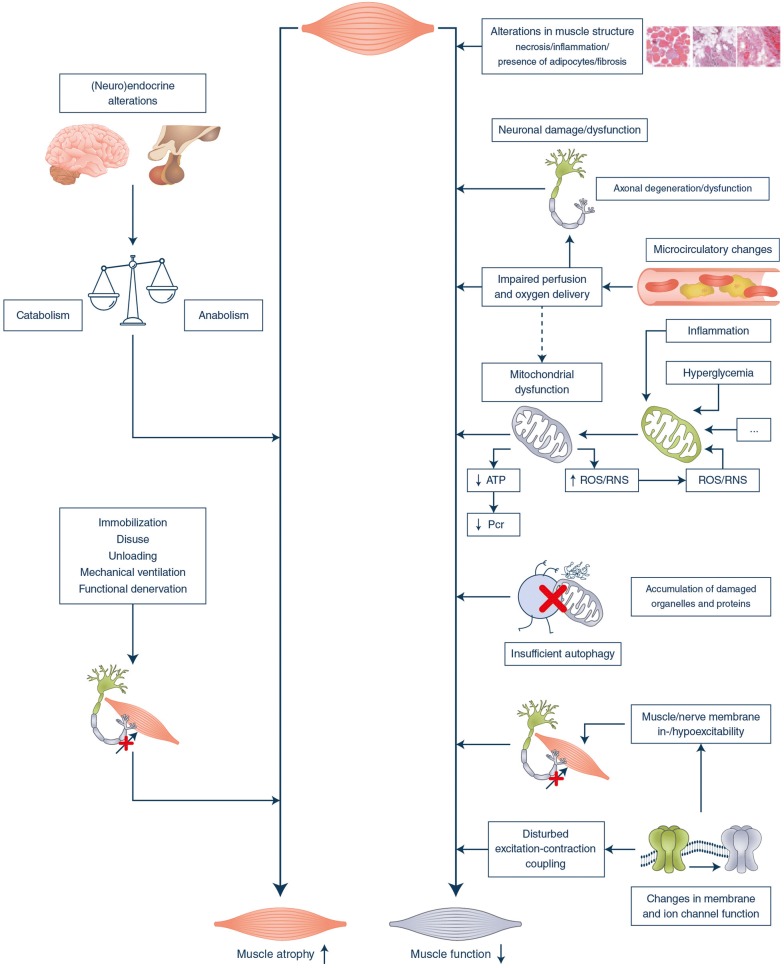
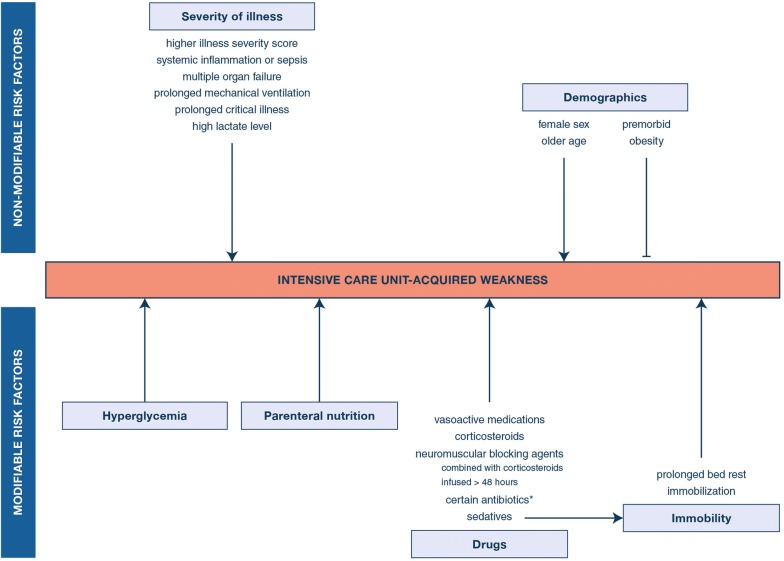
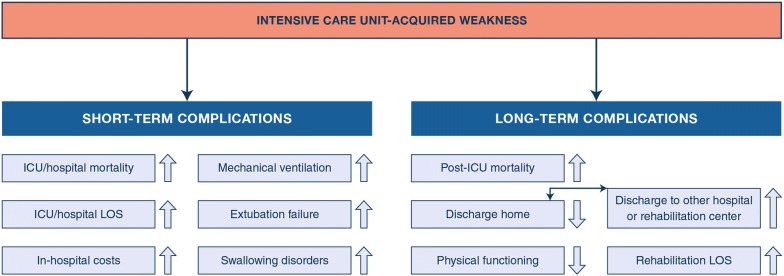
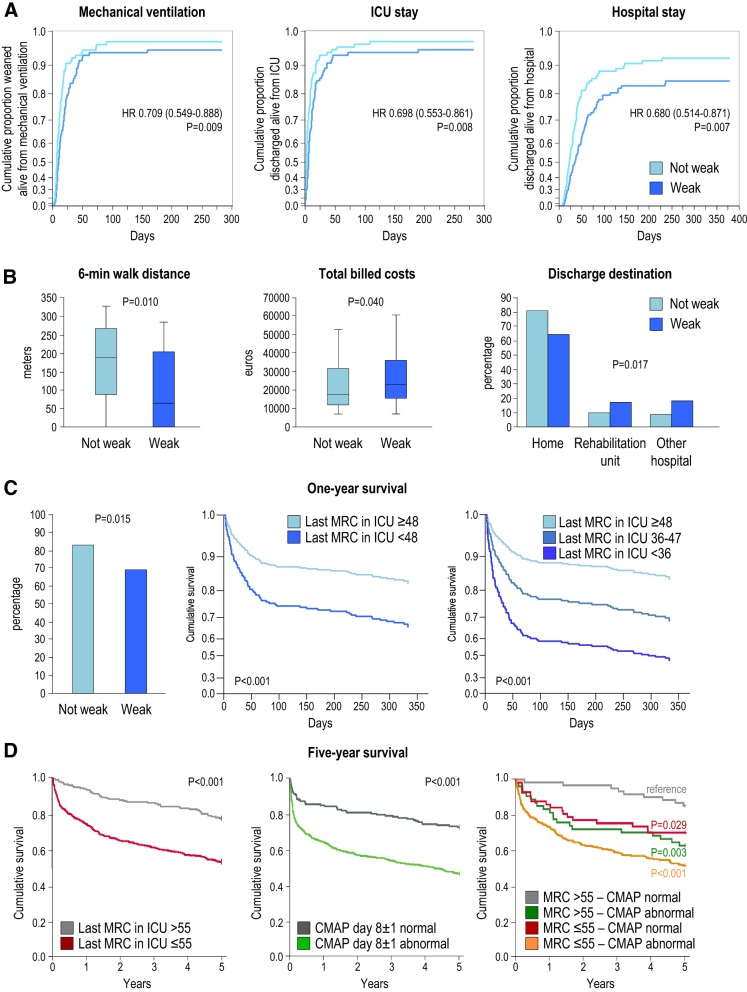
Critically ill patients often acquire neuropathy and/or myopathy labeled ICU-acquired weakness. The current insights into incidence, pathophysiology, diagnostic tools, risk factors, short- and long-term consequences and management of ICU-acquired weakness are narratively reviewed. PubMed was searched for combinations of "neuropathy", "myopathy", "neuromyopathy", or "weakness" with "critical illness", "critically ill", "ICU", "PICU", "sepsis" or "burn". ICU-acquired weakness affects limb and respiratory muscles with a widely varying prevalence depending on the study population. Pathophysiology remains incompletely understood but comprises complex structural/functional alterations within myofibers and neurons. Clinical and electrophysiological tools are used for diagnosis, each with advantages and limitations. Risk factors include age, weight, comorbidities, illness severity, organ failure, exposure to drugs negatively affecting myofibers and neurons, immobility and other intensive care-related factors. ICU-acquired weakness increases risk of in-ICU, in-hospital and long-term mortality, duration of mechanical ventilation and of hospitalization and augments healthcare-related costs, increases likelihood of prolonged care in rehabilitation centers and reduces physical function and quality of life in the long term. RCTs have shown preventive impact of avoiding hyperglycemia, of omitting early parenteral nutrition use and of minimizing sedation. Results of studies investigating the impact of early mobilization, neuromuscular electrical stimulation and of pharmacological interventions were inconsistent, with recent systematic reviews/meta-analyses revealing no or only low-quality evidence for benefit. ICU-acquired weakness predisposes to adverse short- and long-term outcomes. Only a few preventive, but no therapeutic, strategies exist. Further mechanistic research is needed to identify new targets for interventions to be tested in adequately powered RCTs.
Keywords: Clinical outcome; Critical illness; Diagnosis; Intervention; Muscle weakness; Risk factors.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Damian MS, Wijdicks EFM. The clinical management of neuromuscular disorders in intensive care. Neuromuscul Disord. 2019;29:85–96. - PubMed
-
- Stevens RD, Marshall SA, Cornblath DR, Hoke A, Needham DM, de Jonghe B, Ali NA, Sharshar T. A framework for diagnosing and classifying intensive care unit-acquired weakness. Crit Care Med. 2009;37:S299–S308. - PubMed
-
- Latronico N, Herridge M, Hopkins RO, Angus D, Hart N, Hermans G, Iwashyna T, Arabi Y, Citerio G, Ely EW, Hall J, Mehta S, Puntillo K, Van den Hoeven J, Wunsch H, Cook D, Dos Santos C, Rubenfeld G, Vincent JL, Van den Berghe G, Azoulay E, Needham DM. The ICM research agenda on intensive care unit-acquired weakness. Intensive Care Med. 2017;43:1270–1281. - PubMed
-
- Latronico N, Bolton CF. Critical illness polyneuropathy and myopathy: a major cause of muscle weakness and paralysis. Lancet Neurol. 2011;10:931–941. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
