

Interpretations of and management actions following ECGs in programmatic cardiovascular care in primary care: A retrospective dossier study
- PMID: 32077061
- PMCID: PMC7113334
- DOI: 10.1007/s12471-020-01376-3
Interpretations of and management actions following ECGs in programmatic cardiovascular care in primary care: A retrospective dossier study
Abstract
Background: The usefulness of routine electrocardiograms (ECGs) in cardiovascular risk management (CVRM) and diabetes care is doubted.
Objectives: To assess the performance of general practitioners (GPs) in embedding ECGs in CVRM and diabetes care.
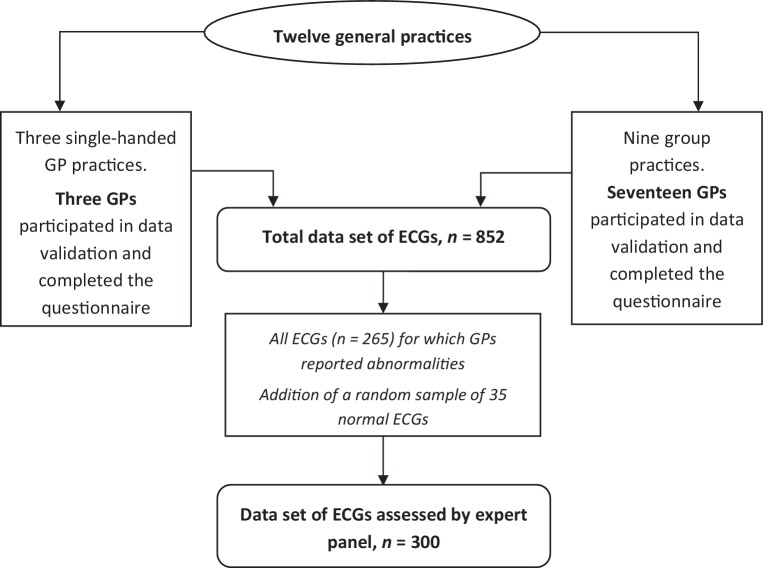
Methods: We collected 852 ECGs recorded by 20 GPs (12 practices) in the context of CVRM and diabetes care. Of all abnormal (n = 265) and a sample of the normal (n = 35) ECGs, data on the indications, interpretations and management actions were extracted from the corresponding medical records. An expert panel consisting of one cardiologist and one expert GP reviewed these 300 ECG cases.
Results: GPs found new abnormalities in 13.0% of all 852 ECGs (12.0% in routinely recorded ECGs versus 24.3% in ECGs performed for a specific indication). Management actions followed more often after ECGs performed for specific indications (17.6%) than after routine ECGs (6.0%). The expert panel agreed with the GPs' interpretations in 67% of the 300 assessed cases. Most often misinterpreted relevant ECG abnormalities were previous myocardial infarction, R‑wave abnormalities and typical/atypical ST-segment and T‑wave (ST-T) abnormalities. Agreement on patient management between GP and expert panel was 74%. Disagreement in most cases concerned additional diagnostic testing.
Conclusions: In the context of programmatic CVRM and diabetes care by GPs, the yield of newly found ECG abnormalities is modest. It is higher for ECGs recorded for a specific reason. Educating GPs seems necessary in this field since they perform less well in interpreting and managing CVRM ECGs than in ECGs performed in symptomatic patients.
Keywords: Clinical competence; Electrocardiography; General practice; Preventive health services; Quality of health care; Retrospective studies.
Conflict of interest statement
N. Van den Nieuwenhof, R.T.A. Willemsen, K.T.S. Konings and H.E.J.H. Stoffers declare that they have no competing interests.
Figures


References
LinkOut - more resources
Full Text Sources
