

Spinal cord injury and diaphragm neuromotor control
- PMID: 32077350
- PMCID: PMC7176525
- DOI: 10.1080/17476348.2020.1732822
Spinal cord injury and diaphragm neuromotor control
Abstract
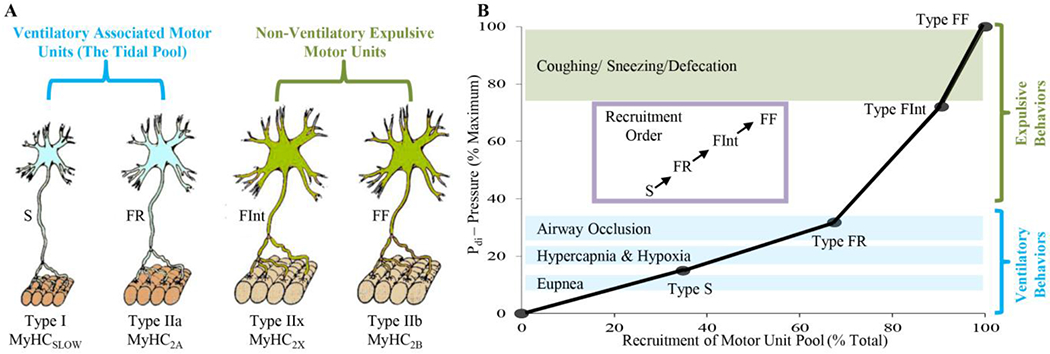
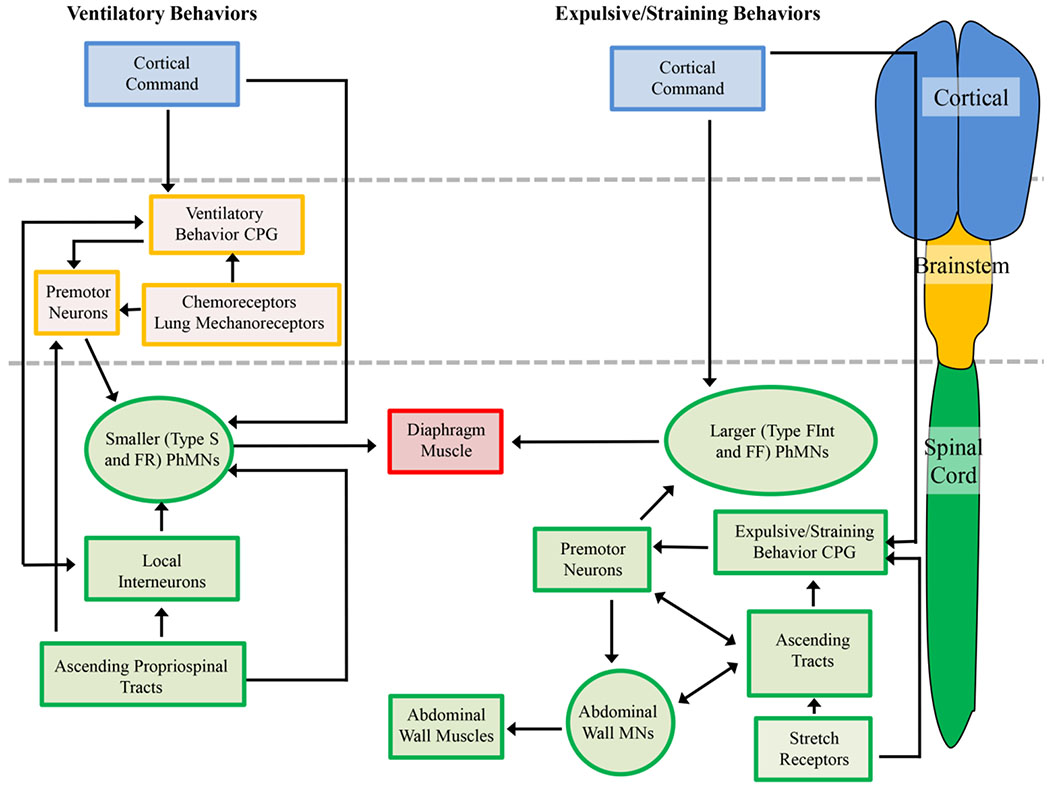
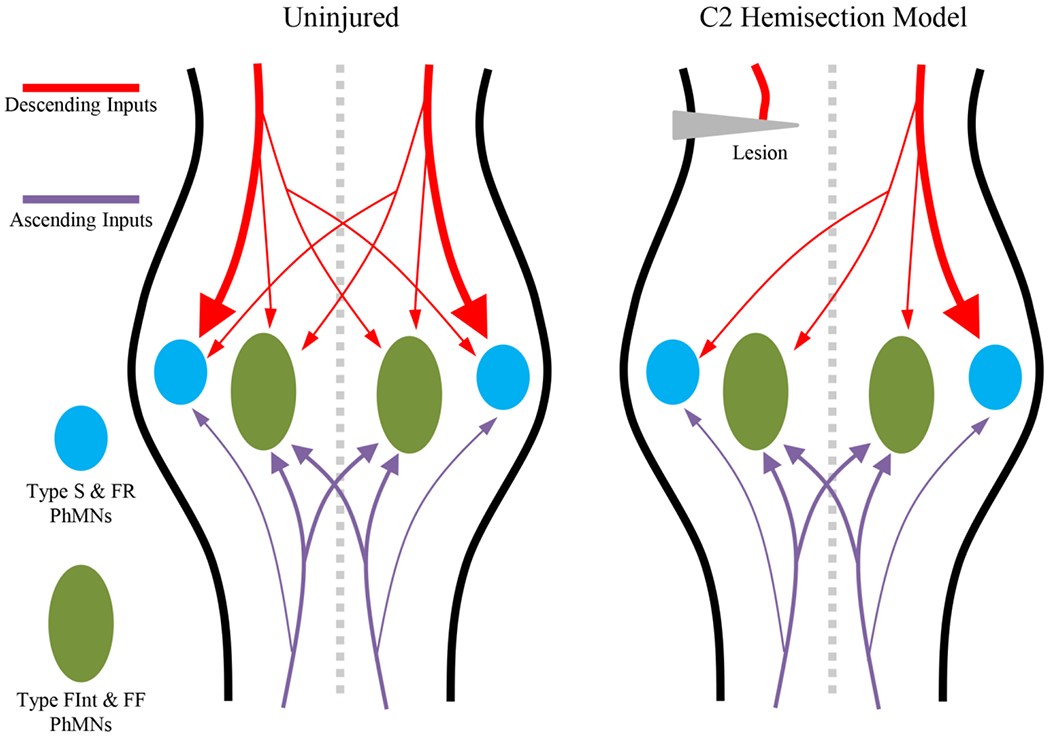
Introduction: Neuromotor control of diaphragm muscle and the recovery of diaphragm activity following spinal cord injury have been narrowly focused on ventilation. By contrast, the understanding of neuromotor control for non-ventilatory expulsive/straining maneuvers (including coughing, defecation, and parturition) is relatively impoverished. This variety of behaviors are achieved via the recruitment of the diverse array of motor units that comprise the diaphragm muscle.Areas covered: The neuromotor control of ventilatory and non-ventilatory behaviors in health and in the context of spinal cord injury is explored. Particular attention is played to the neuroplasticity of phrenic motor neurons in various models of cervical spinal cord injury.Expert opinion: There is a remarkable paucity in our understanding of neuromotor control of maneuvers in spinal cord injury patients. Dysfunction of these expulsive/straining maneuvers reduces patient quality of life and contributes to severe morbidity and mortality. As spinal cord injury patient life expectancies continue to climb steadily, a nexus of spinal cord injury and age-associated comorbidities are likely to occur. While current research remains concerned only with the minutiae of ventilation, the major functional deficits of this clinical cohort will persist intractably. We posit some future research directions to avoid this scenario.
Keywords: Phrenic motor neurons; contusion; hemisection; motor unit; neural circuit; recruitment; skeletal muscle.
Conflict of interest statement
Declaration of interest
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties. The authors have nothing to disclose and declare no actual or perceived conflicts of interest.
Figures
References
-
- Fogarty MJ, Sieck GC. Evolution and Functional Differentiation of the Diaphragm Muscle of Mammals. Compr Physiol. 2019;9(2):715–766. - PMC - PubMed
-
* This review is contains a synthesis of the best information available regarding the ventilatory and non-ventilatory behaviours of the diaphragm muscle.
-
- Sieck GC, Fournier M. Diaphragm motor unit recruitment during ventilatory and nonventilatory behaviors. J Appl Physiol. 1989;66(6):2539–2545. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials