

Initial Precipitants and Recurrence of Atrial Fibrillation
- PMID: 32078361
- PMCID: PMC7141776
- DOI: 10.1161/CIRCEP.119.007716
Initial Precipitants and Recurrence of Atrial Fibrillation
Abstract
Background: Atrial fibrillation (AF) may occur after an acute precipitant and subsequently resolve. Management guidelines for AF in these settings are unclear as the risk of recurrent AF and related morbidity is poorly understood. We examined the relations between acute precipitants of AF and long-term recurrence of AF in a clinical setting.
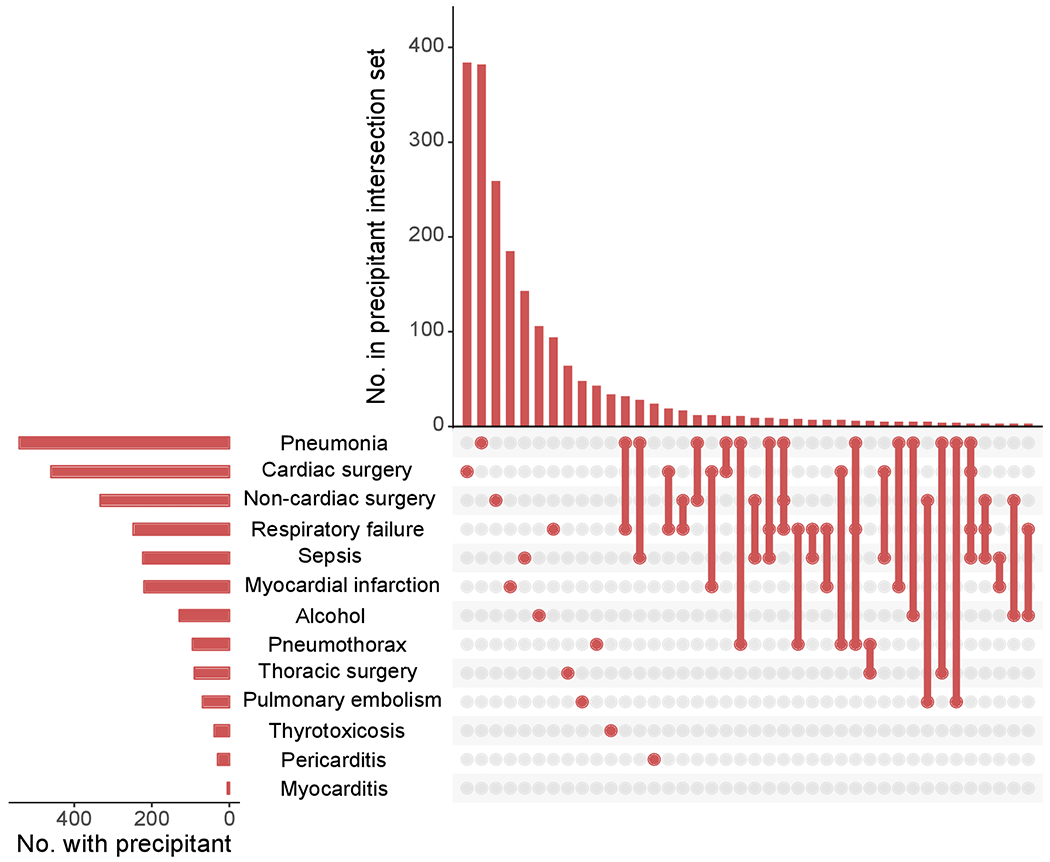
Methods: From a multi-institutional longitudinal electronic medical record database, we identified patients with newly diagnosed AF between 2000 and 2014. We developed algorithms to identify acute AF precipitants (surgery, sepsis, pneumonia, pneumothorax, respiratory failure, myocardial infarction, thyrotoxicosis, alcohol, pericarditis, pulmonary embolism, and myocarditis). We assessed risks of AF recurrence in individuals with and without a precipitant and the relations between AF recurrence and heart failure, stroke, and mortality.
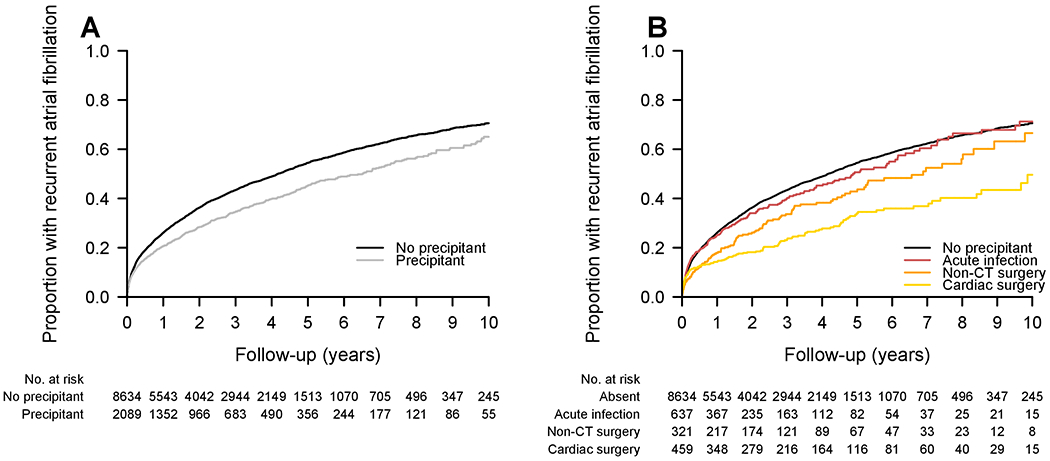
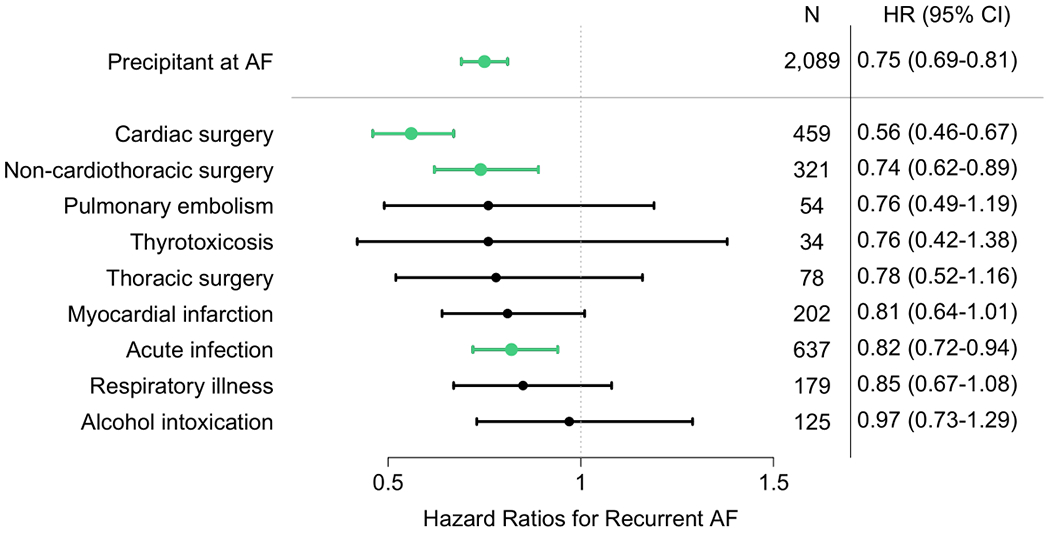
Results: Among 10 723 patients with newly diagnosed AF (67.9±9.9 years, 41% women), 19% had an acute AF precipitant, the most common of which were cardiac surgery (22%), pneumonia (20%), and noncardiothoracic surgery (15%). The cumulative incidence of AF recurrence at 5 years was 41% among individuals with a precipitant compared with 52% in those without a precipitant (adjusted hazard ratio [HR], 0.75 [95% CI, 0.69-0.81]; P<0.001). The lowest risk of recurrence among those with precipitants occurred with postoperative AF (5-year incidence 32% in cardiac surgery and 39% in noncardiothoracic surgery). Regardless of the presence of an initial precipitant, recurrent AF was associated with increased adjusted risks of heart failure (hazard ratio, 2.74 [95% CI, 2.39-3.15]; P<0.001), stroke (hazard ratio, 1.57 [95% CI, 1.30-1.90]; P<0.001), and mortality (hazard ratio, 2.96 [95% CI, 2.70-3.24]; P<0.001).
Conclusions: AF after an acute precipitant frequently recurs, although the risk of recurrence is lower than among individuals without an acute precipitant. Recurrence is associated with substantial long-term morbidity and mortality. Future studies should address surveillance and management after newly diagnosed AF in the setting of an acute precipitant.
Keywords: atrial fibrillation; heart failure; mortality; risk factor; stroke.
Figures
References
Publication types
MeSH terms
Grants and funding
- P50 HL120163/HL/NHLBI NIH HHS/United States
- R01 HL137734/HL/NHLBI NIH HHS/United States
- K24 HL105780/HL/NHLBI NIH HHS/United States
- R01 HL141434/HL/NHLBI NIH HHS/United States
- R01 HL104156/HL/NHLBI NIH HHS/United States
- R01 HL092577/HL/NHLBI NIH HHS/United States
- R01 HL136660/HL/NHLBI NIH HHS/United States
- R21 AG060529/AG/NIA NIH HHS/United States
- R01 HL128914/HL/NHLBI NIH HHS/United States
- R01 HL135219/HL/NHLBI NIH HHS/United States
- T32 HL007208/HL/NHLBI NIH HHS/United States
- 2017039/DDCF/Doris Duke Charitable Foundation/United States
- U54 HL143541/HL/NHLBI NIH HHS/United States
- R01 HL137794/HL/NHLBI NIH HHS/United States
- R01 HL126911/HL/NHLBI NIH HHS/United States
- R01 HL139731/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
