

The Prognostic Significance of Quantitative Myocardial Perfusion: An Artificial Intelligence-Based Approach Using Perfusion Mapping
- PMID: 32078380
- PMCID: PMC7176346
- DOI: 10.1161/CIRCULATIONAHA.119.044666
The Prognostic Significance of Quantitative Myocardial Perfusion: An Artificial Intelligence-Based Approach Using Perfusion Mapping
Abstract
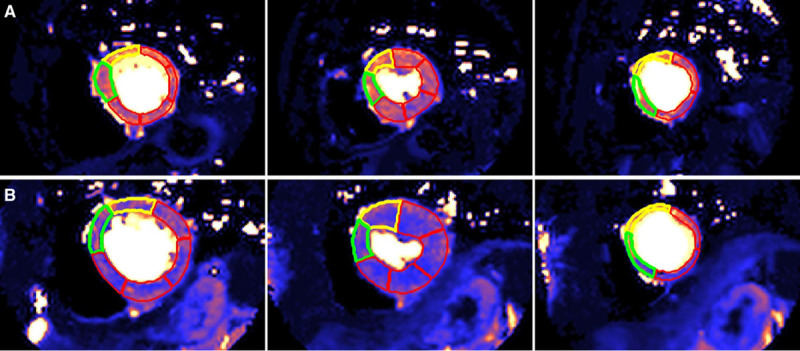
Background: Myocardial perfusion reflects the macro- and microvascular coronary circulation. Recent quantitation developments using cardiovascular magnetic resonance perfusion permit automated measurement clinically. We explored the prognostic significance of stress myocardial blood flow (MBF) and myocardial perfusion reserve (MPR, the ratio of stress to rest MBF).
Methods: A 2-center study of patients with both suspected and known coronary artery disease referred clinically for perfusion assessment. Image analysis was performed automatically using a novel artificial intelligence approach deriving global and regional stress and rest MBF and MPR. Cox proportional hazard models adjusting for comorbidities and cardiovascular magnetic resonance parameters sought associations of stress MBF and MPR with death and major adverse cardiovascular events (MACE), including myocardial infarction, stroke, heart failure hospitalization, late (>90 day) revascularization, and death.
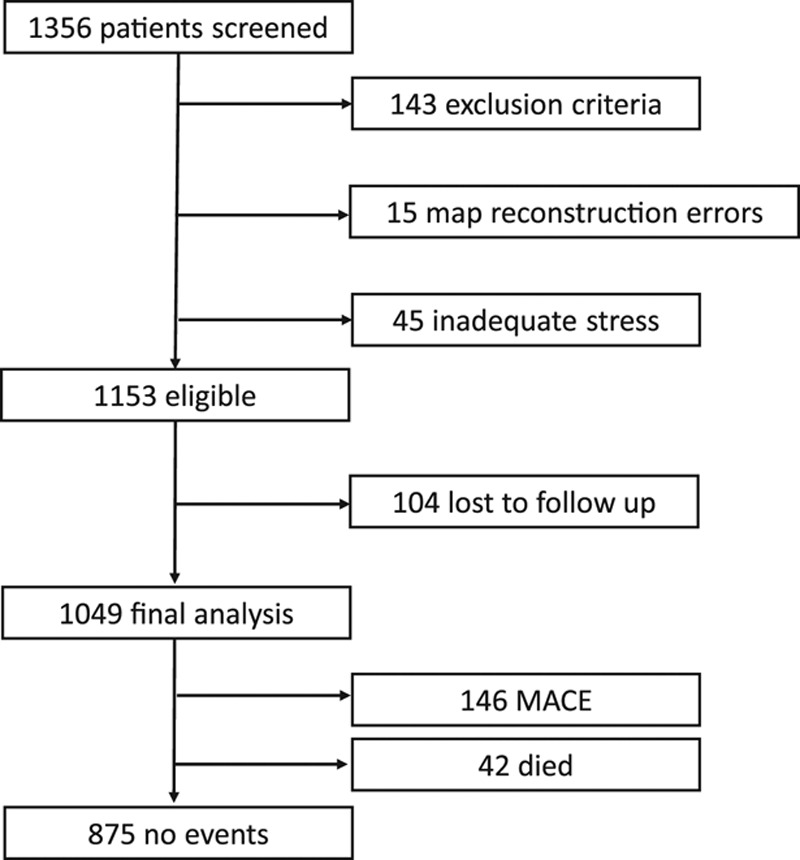
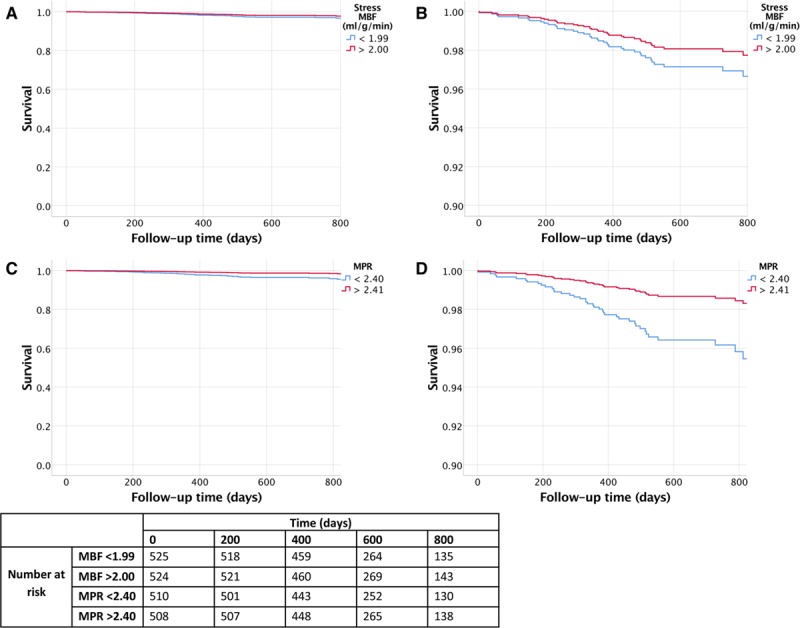
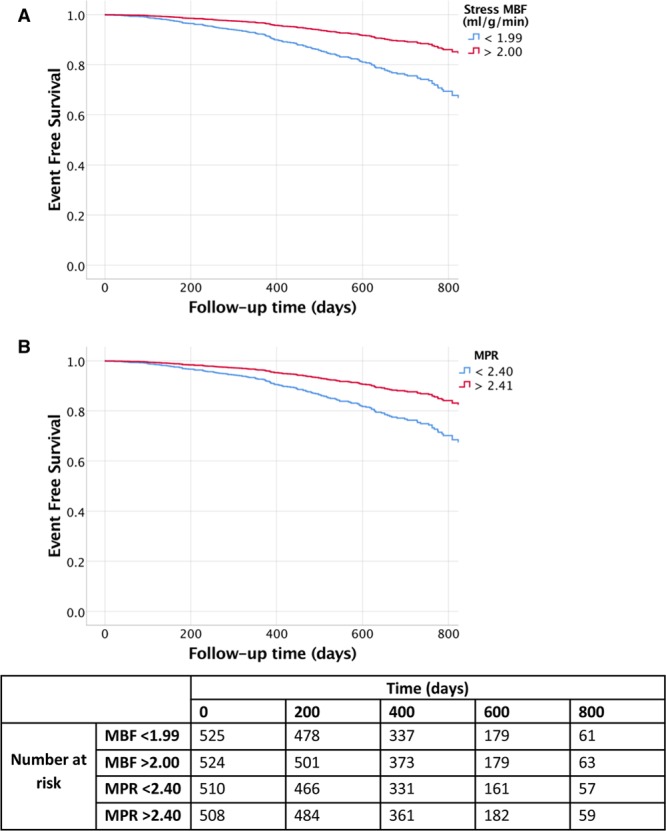
Results: A total of 1049 patients were included with a median follow-up of 605 (interquartile range, 464-814) days. There were 42 (4.0%) deaths and 188 MACE in 174 (16.6%) patients. Stress MBF and MPR were independently associated with both death and MACE. For each 1 mL·g-1·min-1 decrease in stress MBF, the adjusted hazard ratios for death and MACE were 1.93 (95% CI, 1.08-3.48, P=0.028) and 2.14 (95% CI, 1.58-2.90, P<0.0001), respectively, even after adjusting for age and comorbidity. For each 1 U decrease in MPR, the adjusted hazard ratios for death and MACE were 2.45 (95% CI, 1.42-4.24, P=0.001) and 1.74 (95% CI, 1.36-2.22, P<0.0001), respectively. In patients without regional perfusion defects on clinical read and no known macrovascular coronary artery disease (n=783), MPR remained independently associated with death and MACE, with stress MBF remaining associated with MACE only.
Conclusions: In patients with known or suspected coronary artery disease, reduced MBF and MPR measured automatically inline using artificial intelligence quantification of cardiovascular magnetic resonance perfusion mapping provides a strong, independent predictor of adverse cardiovascular outcomes.
Keywords: cardiovascular magnetic resonance; cardiovascular outcomes; inline perfusion quantification; myocardial perfusion.
Figures
Comment in
-
Global Developments in Stress Perfusion Cardiovascular Magnetic Resonance.Circulation. 2020 Apr 21;141(16):1292-1294. doi: 10.1161/CIRCULATIONAHA.120.045967. Epub 2020 Apr 20. Circulation. 2020. PMID: 32310697 Free PMC article. No abstract available.
References
-
- Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, Prescott E, Storey R, Deaton C, Cuisset T, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes: The Task Force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology (ESC). Eur Heart J. 2019;41:407–477. doi: 10.1093/eurheartj/ehz425. - PubMed
-
- Pepine CJ, Anderson RD, Sharaf BL, Reis SE, Smith KM, Handberg EM, Johnson BD, Sopko G, Bairey Merz CN. Coronary microvascular reactivity to adenosine predicts adverse outcome in women evaluated for suspected ischemia results from the National Heart, Lung and Blood Institute WISE (Women’s Ischemia Syndrome Evaluation) study. J Am Coll Cardiol. 2010;55:2825–2832. doi: 10.1016/j.jacc.2010.01.054. - PMC - PubMed
-
- Ford TJ, Stanley B, Good R, Rocchiccioli P, McEntegart M, Watkins S, Eteiba H, Shaukat A, Lindsay M, Robertson K, et al. Stratified medical therapy using invasive coronary function testing in angina: the CorMicA trial. J Am Coll Cardiol. 2018;72(23 p)(t A):2841–2855. doi: 10.1016/j.jacc.2018.09.006. - PubMed
-
- Tonino PA, De Bruyne B, Pijls NH, Siebert U, Ikeno F, van’ t Veer M, Klauss V, Manoharan G, Engstrøm T, Oldroyd KG, et al. FAME Study Investigators. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360:213–224. doi: 10.1056/NEJMoa0807611. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
