

Noninvasive In Vivo Assessment of Cardiac Metabolism in the Healthy and Diabetic Human Heart Using Hyperpolarized 13C MRI
- PMID: 32078413
- PMCID: PMC7077975
- DOI: 10.1161/CIRCRESAHA.119.316260
Noninvasive In Vivo Assessment of Cardiac Metabolism in the Healthy and Diabetic Human Heart Using Hyperpolarized 13C MRI
Abstract
Rationale: The recent development of hyperpolarized 13C magnetic resonance spectroscopy has made it possible to measure cellular metabolism in vivo, in real time.
Objective: By comparing participants with and without type 2 diabetes mellitus (T2DM), we report the first case-control study to use this technique to record changes in cardiac metabolism in the healthy and diseased human heart.
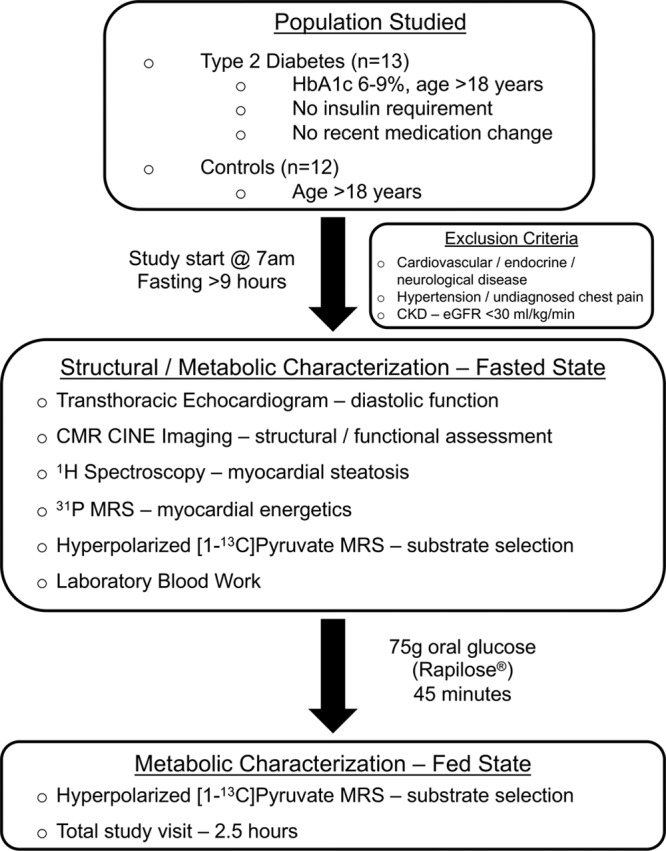
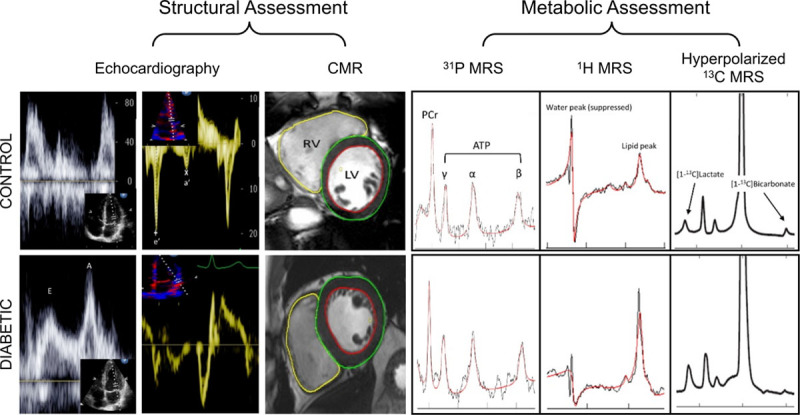
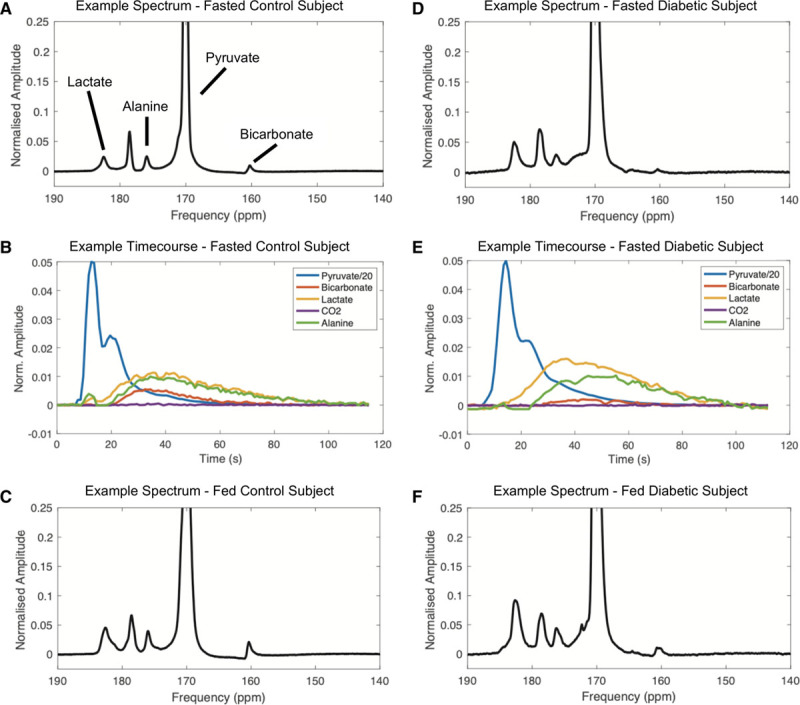
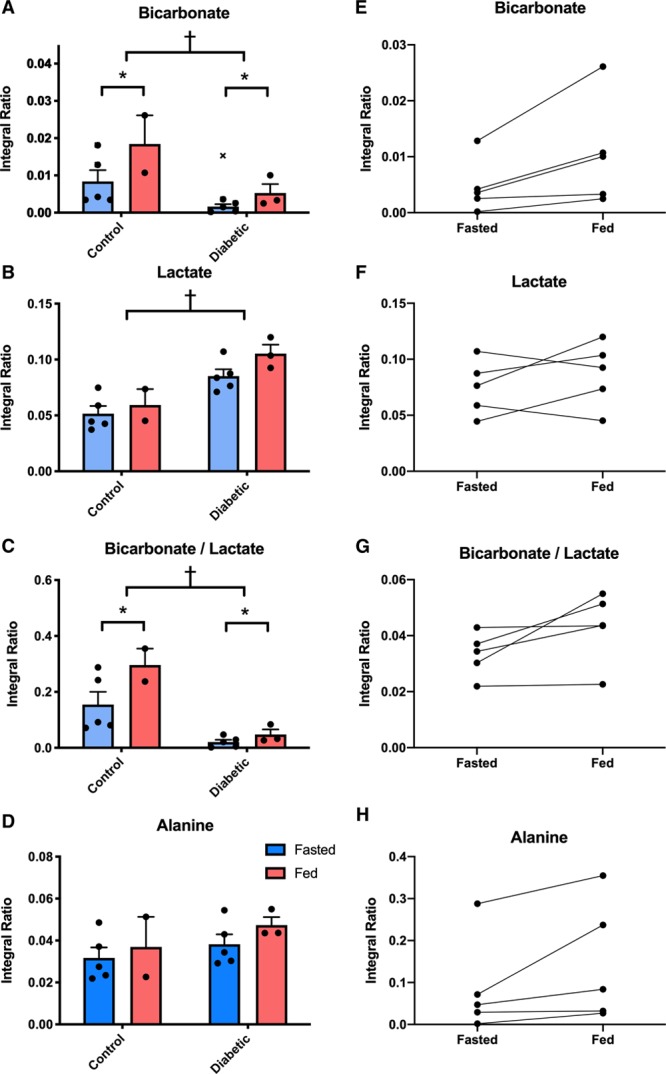
Methods and results: Thirteen people with T2DM (glycated hemoglobin, 6.9±1.0%) and 12 age-matched healthy controls underwent assessment of cardiac systolic and diastolic function, myocardial energetics (31P-magnetic resonance spectroscopy), and lipid content (1H-magnetic resonance spectroscopy) in the fasted state. In a subset (5 T2DM, 5 control), hyperpolarized [1-13C]pyruvate magnetic resonance spectra were also acquired and in 5 of these participants (3 T2DM, 2 controls), this was successfully repeated 45 minutes after a 75 g oral glucose challenge. Downstream metabolism of [1-13C]pyruvate via PDH (pyruvate dehydrogenase, [13C]bicarbonate), lactate dehydrogenase ([1-13C]lactate), and alanine transaminase ([1-13C]alanine) was assessed. Metabolic flux through cardiac PDH was significantly reduced in the people with T2DM (Fasted: 0.0084±0.0067 [Control] versus 0.0016±0.0014 [T2DM], Fed: 0.0184±0.0109 versus 0.0053±0.0041; P=0.013). In addition, a significant increase in metabolic flux through PDH was observed after the oral glucose challenge (P<0.001). As is characteristic of diabetes mellitus, impaired myocardial energetics, myocardial lipid content, and diastolic function were also demonstrated in the wider study cohort.
Conclusions: This work represents the first demonstration of the ability of hyperpolarized 13C magnetic resonance spectroscopy to noninvasively assess physiological and pathological changes in cardiac metabolism in the human heart. In doing so, we highlight the potential of the technique to detect and quantify metabolic alterations in the setting of cardiovascular disease.
Keywords: diabetes mellitus; diabetic cardiomyopathy; hyperpolarized magnetic resonance spectroscopy; magnetic resonance imaging; metabolism; pyruvate dehydrogenase.
Figures
References
-
- Adams KF, Schatzkin A, Harris TB, Kipnis V, Mouw T, Ballard-Barbash R, Hollenbeck A, Leitzmann MF. Overweight, obesity, and mortality in a large prospective cohort of persons 50 to 71 years old. N Engl J Med. 2006;355:763–778. doi: 10.1056/NEJMoa055643. - PubMed
-
- Heather LC, Clarke K. Metabolism, hypoxia and the diabetic heart. J Mol Cell Cardiol. 2011;50:598–605. doi: 10.1016/j.yjmcc.2011.01.007. - PubMed
-
- Randle PJ, Kerbey AL, Espinal J. Mechanisms decreasing glucose oxidation in diabetes and starvation: role of lipid fuels and hormones. Diabetes Metab Rev. 1988;4:623–638. doi: 10.1002/dmr.5610040702. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- FS/15/80/31803/BHF_/British Heart Foundation/United Kingdom
- RG/11/9/28921/BHF_/British Heart Foundation/United Kingdom
- RE/08/004/23915/BHF_/British Heart Foundation/United Kingdom
- G0601490/MRC_/Medical Research Council/United Kingdom
- RE/13/1/30181/BHF_/British Heart Foundation/United Kingdom
- FS/14/54/30946/BHF_/British Heart Foundation/United Kingdom
- 17242/CRUK_/Cancer Research UK/United Kingdom
- 27150/CRUK_/Cancer Research UK/United Kingdom
- 16628/CRUK_/Cancer Research UK/United Kingdom
- FS/19/18/34252/BHF_/British Heart Foundation/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- FS/17/18/32449/BHF_/British Heart Foundation/United Kingdom
- FS/14/17/30634/BHF_/British Heart Foundation/United Kingdom
- 16465/CRUK_/Cancer Research UK/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Research Materials
