

Targeting Age-Related Pathways in Heart Failure
- PMID: 32078451
- PMCID: PMC7041880
- DOI: 10.1161/CIRCRESAHA.119.315889
Targeting Age-Related Pathways in Heart Failure
Abstract
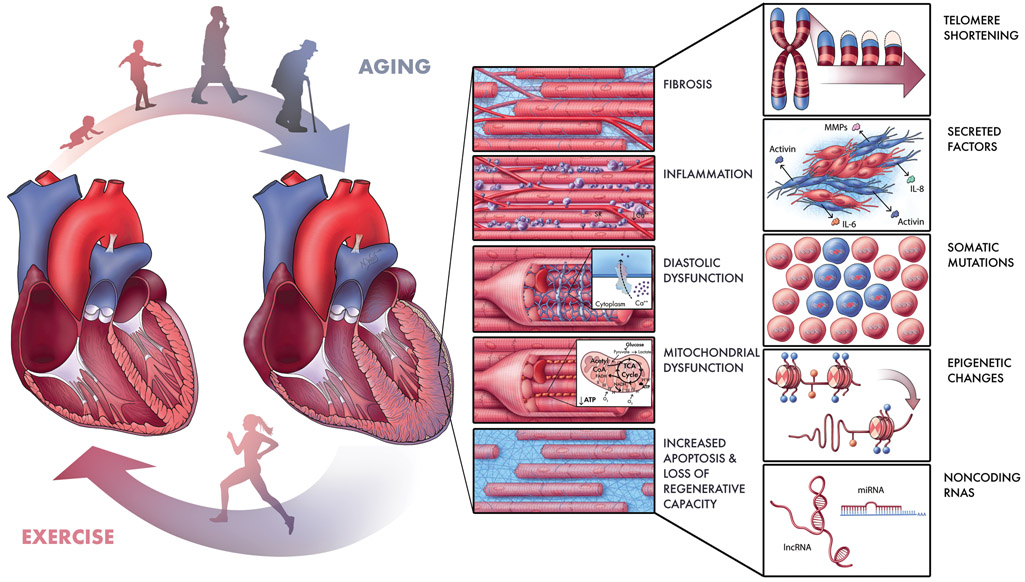
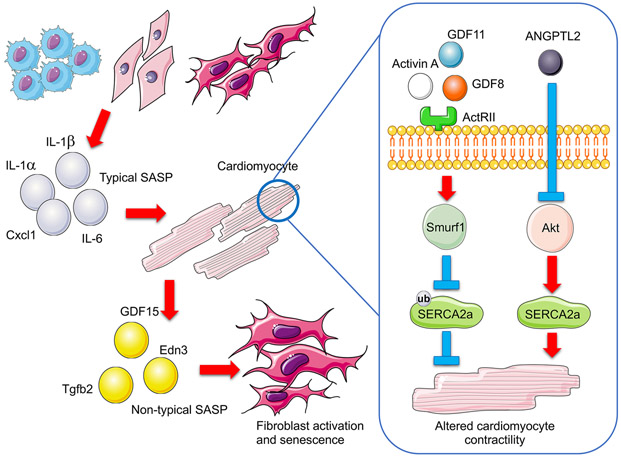
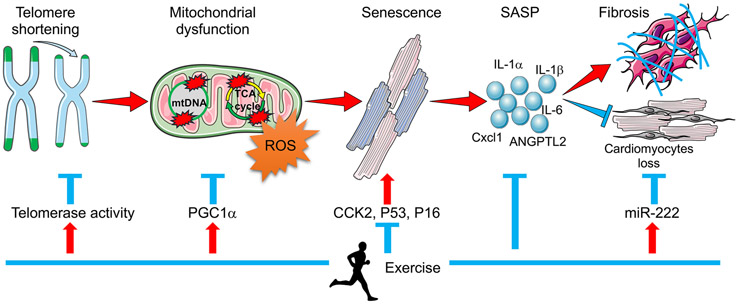
During aging, deterioration in cardiac structure and function leads to increased susceptibility to heart failure. The need for interventions to combat this age-related cardiac decline is becoming increasingly urgent as the elderly population continues to grow. Our understanding of cardiac aging, and aging in general, is limited. However, recent studies of age-related decline and its prevention through interventions like exercise have revealed novel pathological and cardioprotective pathways. In this review, we summarize recent findings concerning the molecular mechanisms of age-related heart failure and highlight exercise as a valuable experimental platform for the discovery of much-needed novel therapeutic targets in this chronic disease.
Keywords: aging; epigenetics; exercise; heart failure; senescence.
Figures
References
-
- Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Das SR, Delling FN, Djousse L, Elkind MSV, Ferguson JF, Fornage M, Jordan LC, Khan SS, Kissela BM, Knutson KL, Kwan TW, Lackland DT, Lewis TT, Lichtman JH, Longenecker CT, Loop MS, Lutsey PL, Martin SS, Matsushita K, Moran AE, Mussolino ME, O’Flaherty M, Pandey A, Perak AM, Rosamond WD, Roth GA, Sampson UKA, Satou GM, Schroeder EB, Shah SH, Spartano NL, Stokes A, Tirschwell DL, Tsao CW, Turakhia MP, VanWagner LB, Wilkins JT, Wong SS, Virani SS, American Heart Association Council on E, Prevention Statistics C, Stroke Statistics S. Heart disease and stroke statistics-2019 update: A report from the american heart association. Circulation. 2019;139:e56–e528 - PubMed
-
- Fleg JL, Cooper LS, Borlaug BA, Haykowsky MJ, Kraus WE, Levine BD, Pfeffer MA, Pina IL, Poole DC, Reeves GR, Whellan DJ, Kitzman DW, National Heart L, Blood Institute Working G. Exercise training as therapy for heart failure: Current status and future directions. Circ Heart Fail. 2015;8:209–220 - PMC - PubMed
-
- Lakatta EG, Levy D. Arterial and cardiac aging: Major shareholders in cardiovascular disease enterprises: Part i: Aging arteries: A “set up” for vascular disease. Circulation. 2003;107:139–146 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
