

Natural History of Cognitive Impairment in Critical Illness Survivors. A Systematic Review
- PMID: 32078780
- PMCID: PMC7365360
- DOI: 10.1164/rccm.201904-0816CI
Natural History of Cognitive Impairment in Critical Illness Survivors. A Systematic Review
Abstract
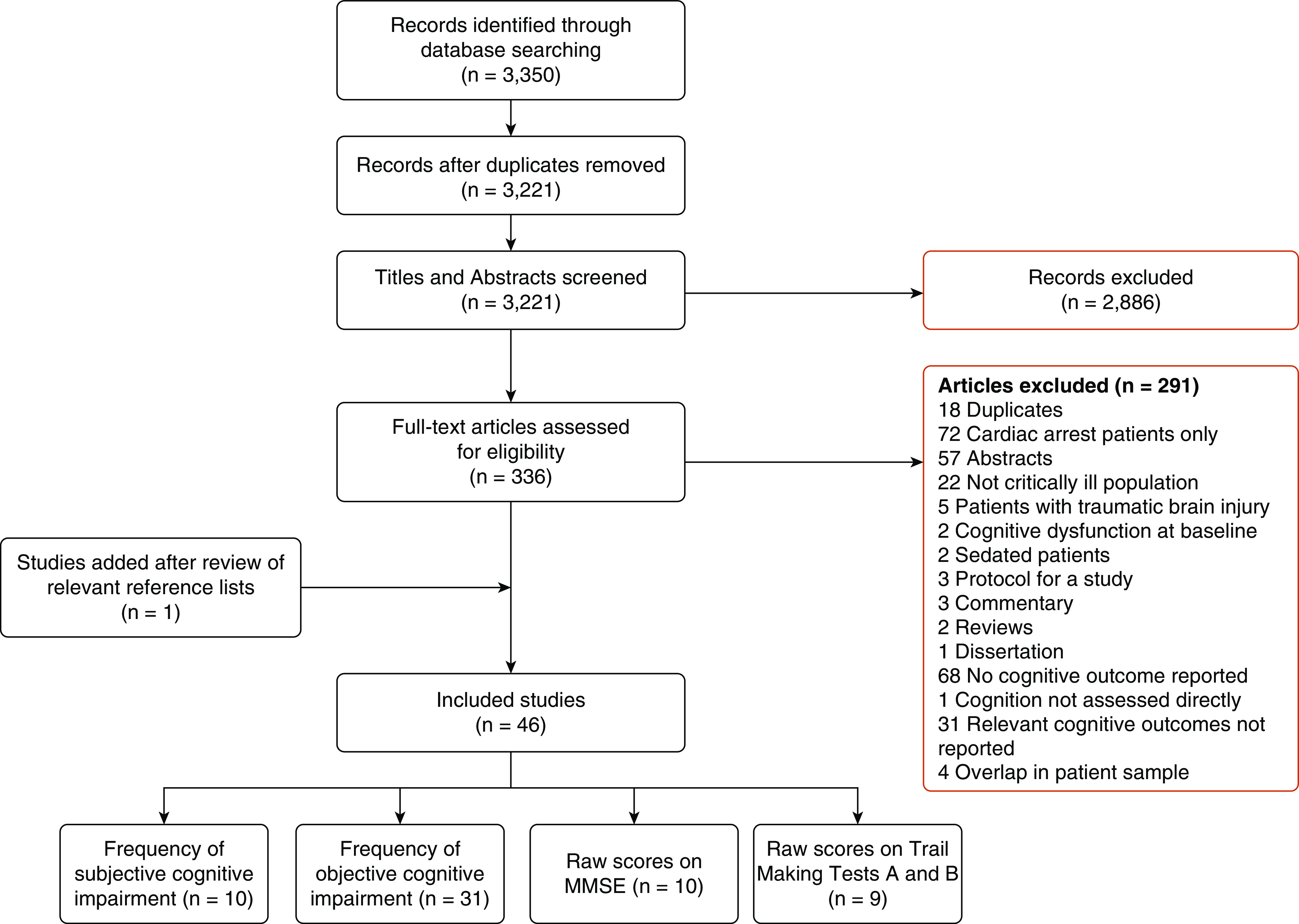
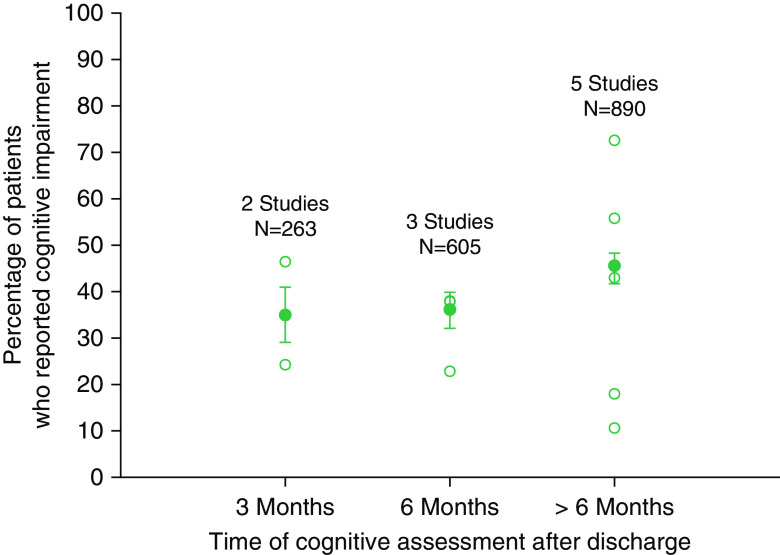
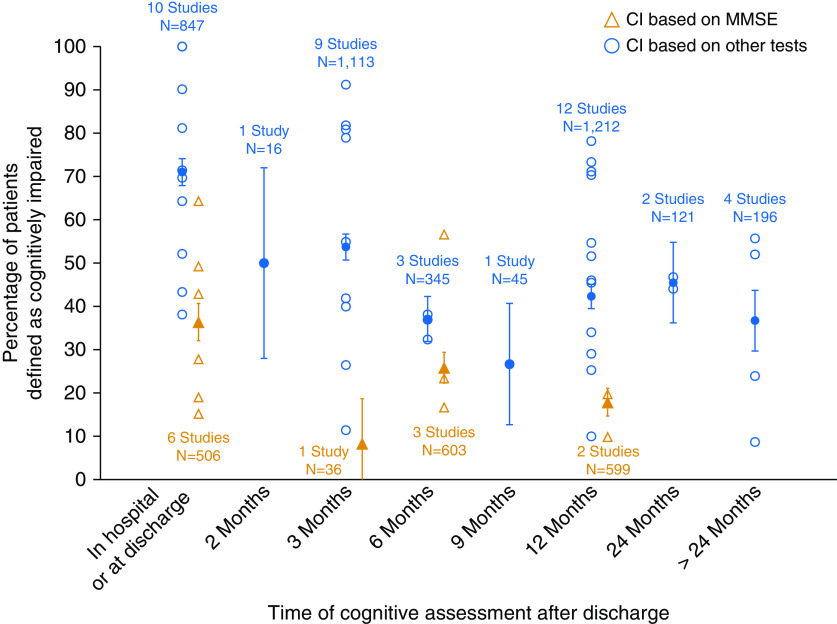
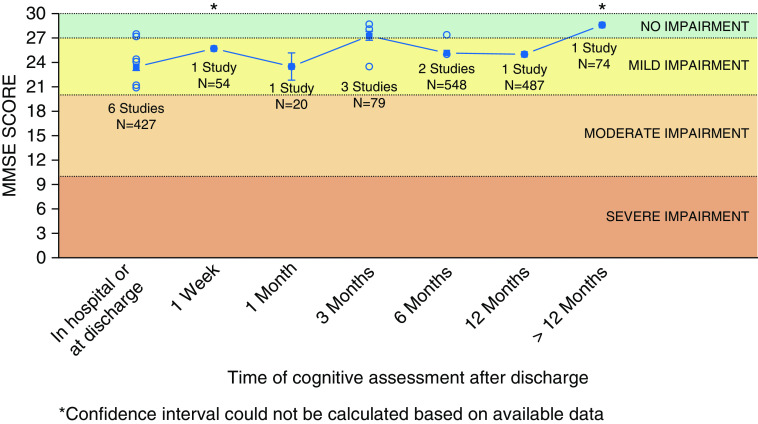
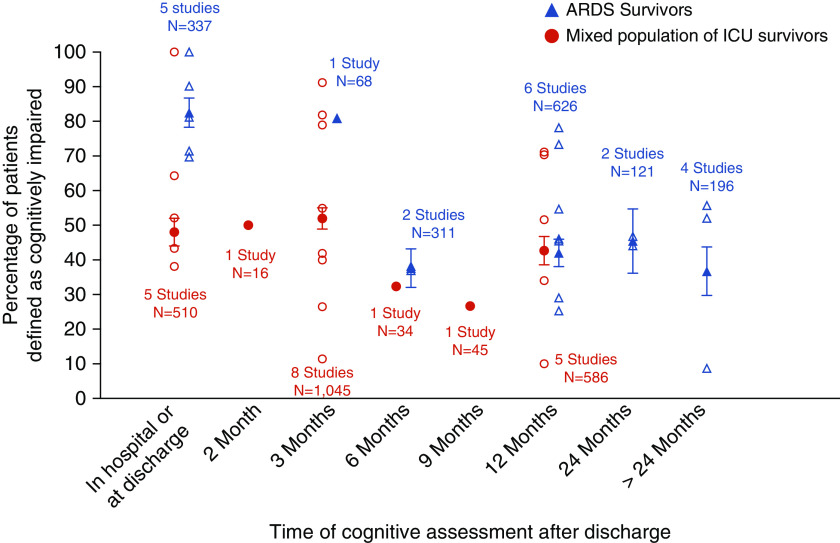
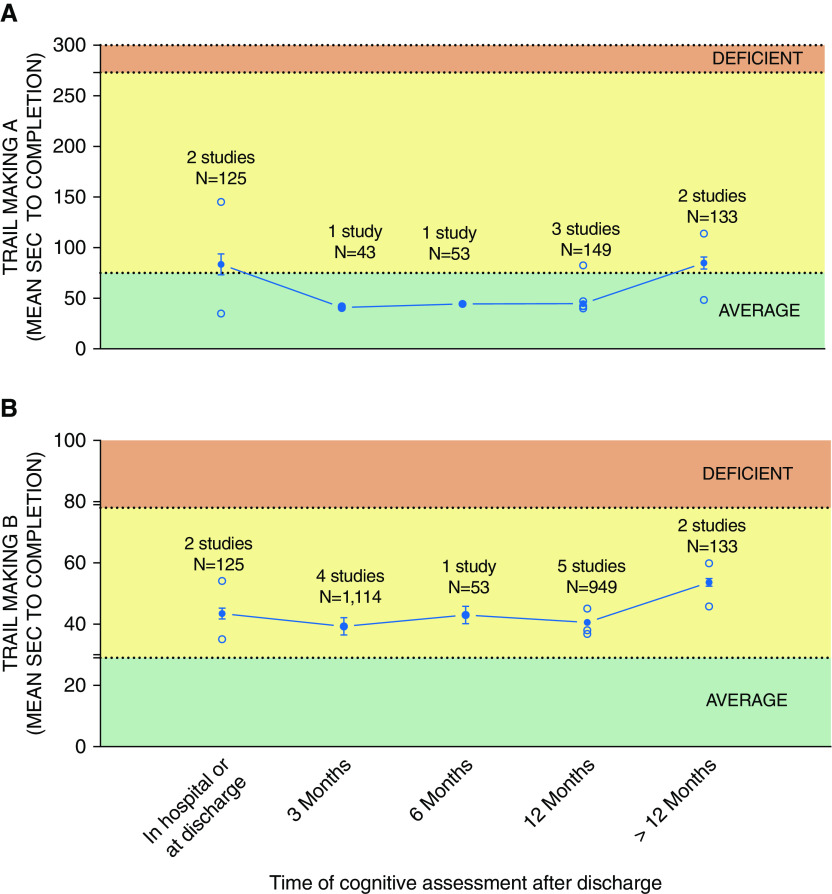
Long-term cognitive impairment is common among ICU survivors, but its natural history remains unclear. In this systematic review, we report the frequency of cognitive impairment in ICU survivors across various time points after ICU discharge that were extracted from 46 of the 3,350 screened records. Prior studies used a range of cognitive instruments, including subjective assessments (10 studies), single or screening cognitive test such as Mini-Mental State Examination or Trail Making Tests A and B (23 studies), and comprehensive cognitive batteries (26 studies). The mean prevalence of cognitive impairment was higher with objective rather than subjective assessments (54% [95% confidence interval (CI), 51-57%] vs. 35% [95% CI, 29-41%] at 3 months after ICU discharge) and when comprehensive cognitive batteries rather than Mini-Mental State Examination were used (ICU discharge: 61% [95% CI, 38-100%] vs. 36% [95% CI, 15-63%]; 12 months after ICU discharge: 43% [95% CI, 10-78%] vs. 18% [95% CI, 10-20%]). Patients with acute respiratory distress syndrome had higher prevalence of cognitive impairment than mixed ICU patients at ICU discharge (82% [95% CI, 78-86%] vs. 48% [95% CI, 44-52%]). Although some studies repeated tests at more than one time point, the time intervals between tests were arbitrary and dictated by operational limitations of individual studies or chosen cognitive instruments. In summary, the prevalence and temporal trajectory of ICU-related cognitive impairment varies depending on the type of cognitive instrument used and the etiology of critical illness. Future studies should use modern comprehensive batteries to better delineate the natural history of cognitive recovery across ICU patient subgroups and determine which acute illness and treatment factors are associated with better recovery trajectories.
Keywords: cognition disorders; cognitive dysfunction; critical care outcomes; critical illness; survivors.
Figures
References
-
- Karnatovskaia LV, Johnson MM, Benzo RP, Gajic O. The spectrum of psychocognitive morbidity in the critically ill: a review of the literature and call for improvement. J Crit Care. 2015;30:130–137. - PubMed
-
- Barr J, Fraser GL, Puntillo K, Ely EW, Gélinas C, Dasta JF, et al. American College of Critical Care Medicine. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med. 2013;41:263–306. - PubMed
-
- Honarmand K, Lalli RL, McIntyre CW, Owen A, Slessarev M. The natural history of cognitive impairment in ICU survivors: a systematic review of the literature. Can J Anesth. 2019;66:1–129.
-
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62:e1–e34. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical