

Independent Blinded Validation of a Tissue Systems Pathology Test to Predict Progression in Patients With Barrett's Esophagus
- PMID: 32079863
- PMCID: PMC7274882
- DOI: 10.14309/ajg.0000000000000556
Independent Blinded Validation of a Tissue Systems Pathology Test to Predict Progression in Patients With Barrett's Esophagus
Abstract
Introduction: A risk prediction test was previously validated to predict progression to high-grade dysplasia (HGD) and esophageal adenocarcinoma (EAC) in patients with Barrett's esophagus (BE). The aim of our study was to independently validate this test to predict the risk of progression to HGD/EAC in BE patients with nondysplastic (ND), indefinite for dysplasia and low-grade dysplasia (LGD).
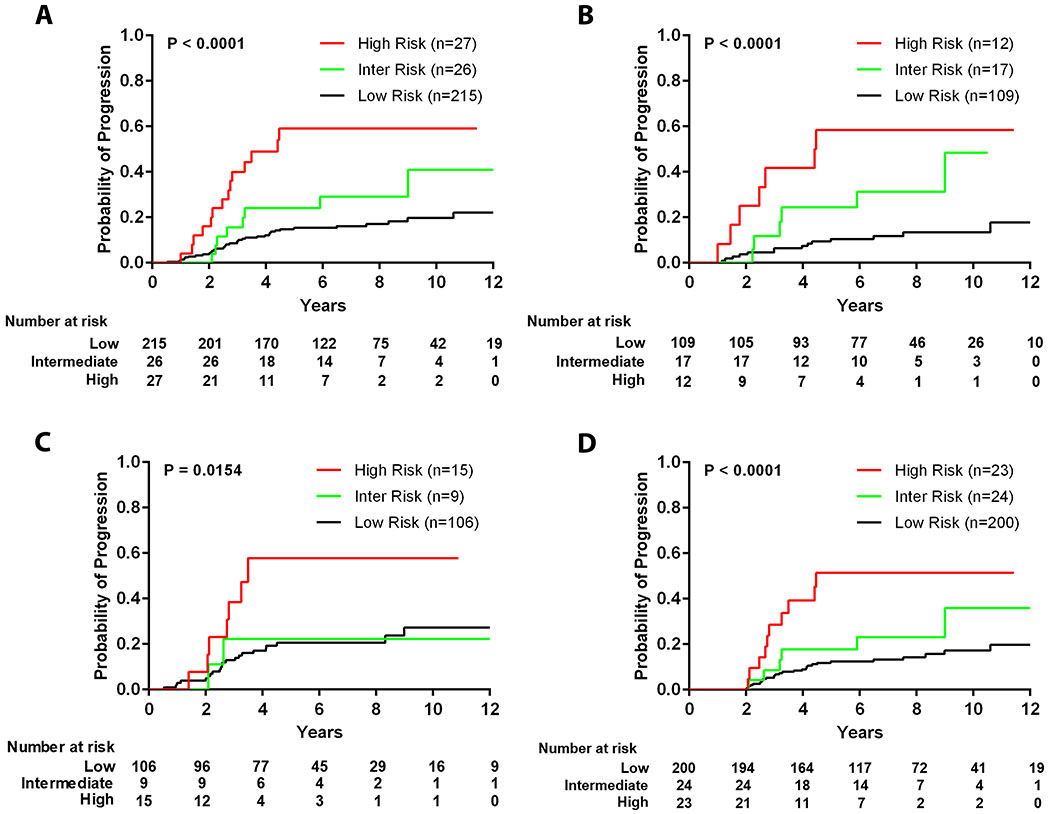
Methods: A single-blinded, case-control study was conducted to stratify patients with BE as low, intermediate, or high risk for progression to HGD/EAC within 5 years using a previously described risk prediction test. Patients with BE who progressed to HGD/EAC after at least 1 year (n = 58) were matched to patients undergoing surveillance without progression (n = 210, median surveillance 7 years). Baseline biopsies with subspecialist diagnoses of ND, indefinite for dysplasia, or LGD were tested in a blinded manner, and the predictive performance of the test was assessed.
Results: This risk prediction test stratified patients with BE based on progression risk with the high-risk group at 4.7-fold increased risk for HGD/EAC compared with the low-risk group (95% confidence interval 2.5-8.8, P < 0.0001). Prevalence-adjusted positive predictive value at 5 years was 23%. The high-risk class and male sex provided predictive power that was independent of pathologic diagnosis, age, segment length, and hiatal hernia. Patients with ND BE who scored high risk progressed at a higher rate (26%) than patients with subspecialist-confirmed LGD (21.8%) at 5 years.
Discussion: A risk prediction test identifies patients with ND BE who are at high risk for progression to HGD/EAC and may benefit from early endoscopic therapy or increased surveillance.
Conflict of interest statement
Potential competing interests:
R.J. Critchley-Thorne has ownership interest (including stock options and patents) in Cernostics, Inc. A.D. DeWard, E.A. Bossart, and S.L. Hayward have ownership interest (including stock options) in Cernostics, Inc. Y. Zhang is a consultant for Cernostics, Inc. There are no relevant conflicts of interest for the other authors.
Figures

Comment in
-
Predicting Progression in Barrett's Esophagus: Is the Holy Grail Within Reach?Am J Gastroenterol. 2020 Jun;115(6):841-842. doi: 10.14309/ajg.0000000000000635. Am J Gastroenterol. 2020. PMID: 32287139 Free PMC article.
References
-
- Wani S, Falk G, Hall M, et al. Patients with nondysplastic Barrett’s esophagus have low risks for developing dysplasia or esophageal adenocarcinoma. Clin Gastroenterol Hepatol 2011;9:220–7; quiz e26. - PubMed
-
- Wani S, Falk GW, Post J, et al. Risk factors for progression of low-grade dysplasia in patients with Barrett’s esophagus. Gastroenterology 2011;141:1179–86, 1186, e1. - PubMed
-
- Desai TK, Krishnan K, Samala N, et al. The incidence of oesophageal adenocarcinoma in non-dysplastic Barrett’s oesophagus: a meta-analysis. Gut 2012;61:970–6. - PubMed
-
- Spechler SJ, Sharma P, Souza RF, et al. American Gastroenterological Association medical position statement on the management of Barrett’s esophagus. Gastroenterology 2011;140:1084–91. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
