Defining the risk of first intravenous immunoglobulin unresponsiveness in non-Asian patients with Kawasaki disease
- PMID: 32080307
- PMCID: PMC7033244
- DOI: 10.1038/s41598-020-59972-7
Defining the risk of first intravenous immunoglobulin unresponsiveness in non-Asian patients with Kawasaki disease
Abstract
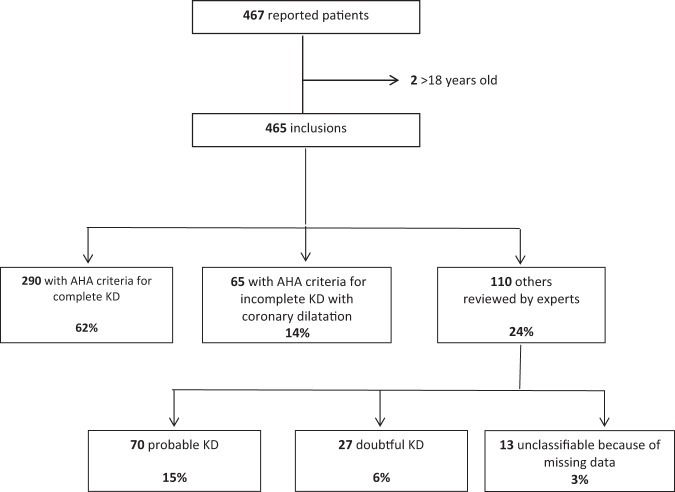
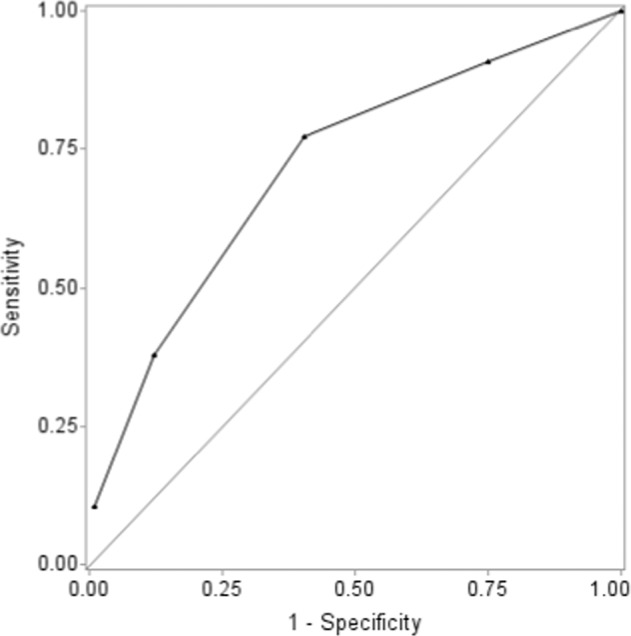
About 10-20% of patients with Kawasaki disease (KD) are unresponsive to intravenous immunoglobulin (IVIg) and are at increased risk of coronary artery abnormalities (CAAs). Early identification is critical to initiate aggressive therapies, but available scoring systems lack sensitivity in non-Japanese populations. We investigated the accuracy of 3 Japanese scoring systems and studied factors associated with IVIg unresponsiveness in a large multiethnic French population of children with KD to build a new scoring system. Children admitted for KD between 2011-2014 in 65 centers were enrolled. Factors associated with second line-treatment; i.e. unresponsiveness to initial IVIg treatment, were analyzed by multivariate regression analysis. The performance of our score and the Kobayashi, Egami and Sano scores were compared in our population and in ethnic subgroups. Overall, 465 children were reported by 84 physicians; 425 were classified with KD (55% European Caucasian, 12% North African/Middle Eastern, 10% African/Afro-Caribbean, 3% Asian and 11% mixed). Eighty patients (23%) needed second-line treatment. Japanese scores had poor performance in our whole population (sensitivity 14-61%). On multivariate regression analysis, predictors of secondary treatment after initial IVIG were hepatomegaly, ALT level ≥30 IU/L, lymphocyte count <2400/mm3 and time to treatment <5 days. The best sensitivity (77%) and specificity (60%) of this model was with 1 point per variable and cut-off ≥2 points. The sensitivity remained good in our 3 main ethnic subgroups (74-88%). We identified predictors of IVIg resistance and built a new score with good sensitivity and acceptable specificity in a non-Asian population.
Conflict of interest statement
The authors declare no competing interests.
Figures