

IL-6-mediated hepatocyte production is the primary source of plasma and urine neutrophil gelatinase-associated lipocalin during acute kidney injury
- PMID: 32081304
- PMCID: PMC8409721
- DOI: 10.1016/j.kint.2019.11.013
IL-6-mediated hepatocyte production is the primary source of plasma and urine neutrophil gelatinase-associated lipocalin during acute kidney injury
Abstract
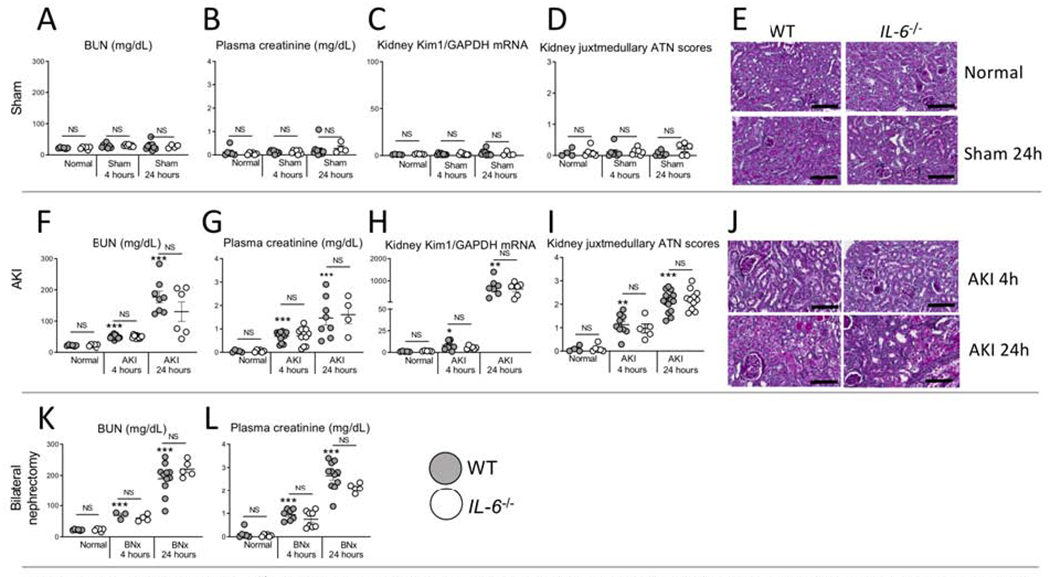
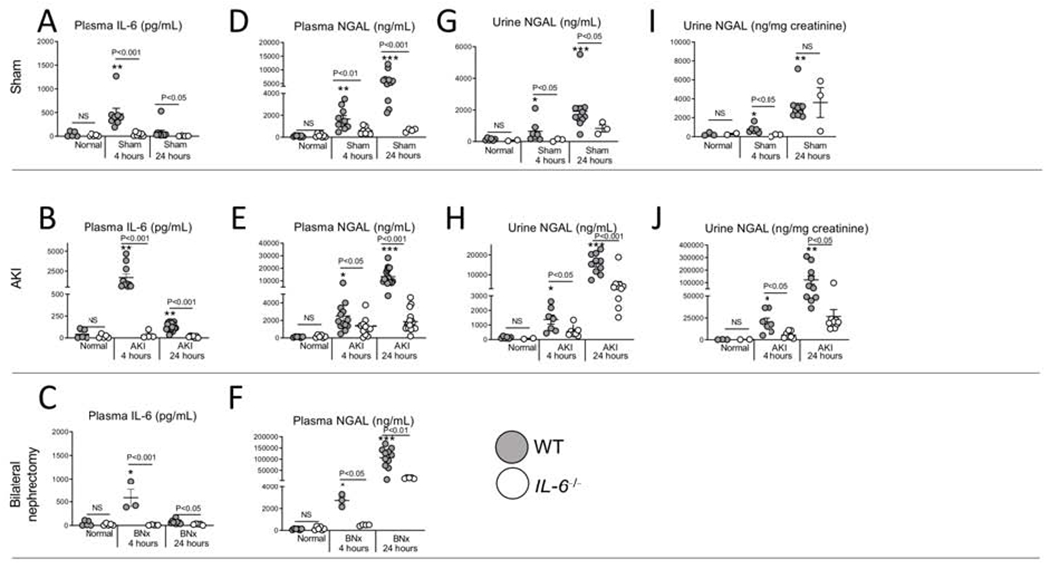
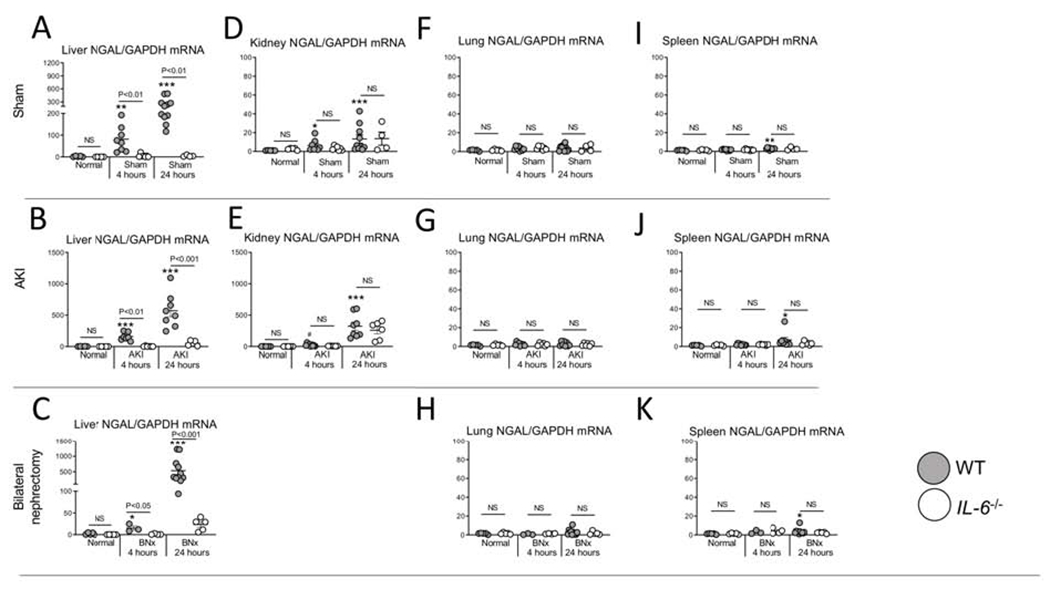
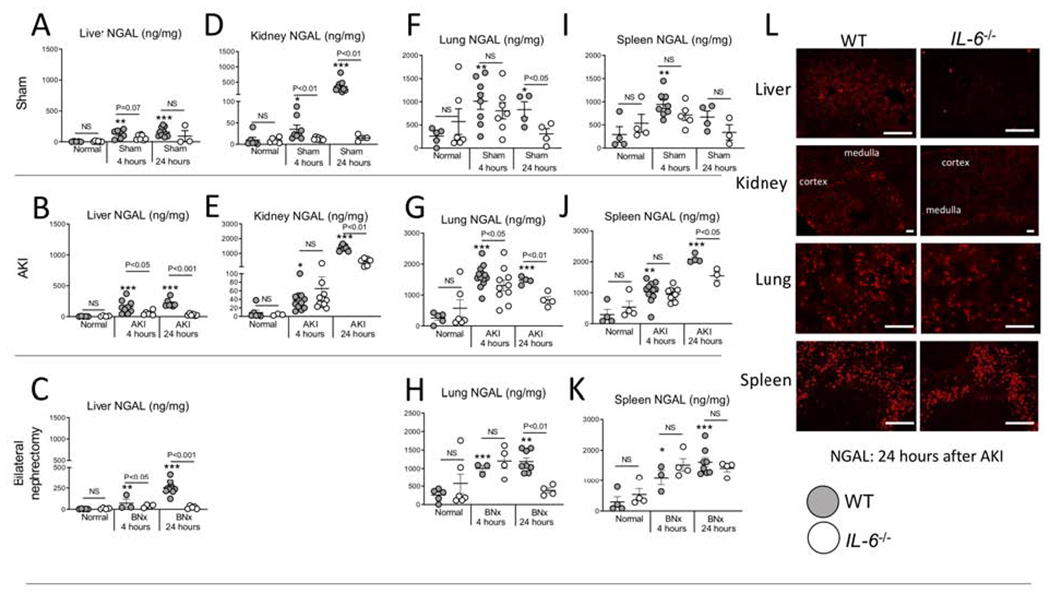
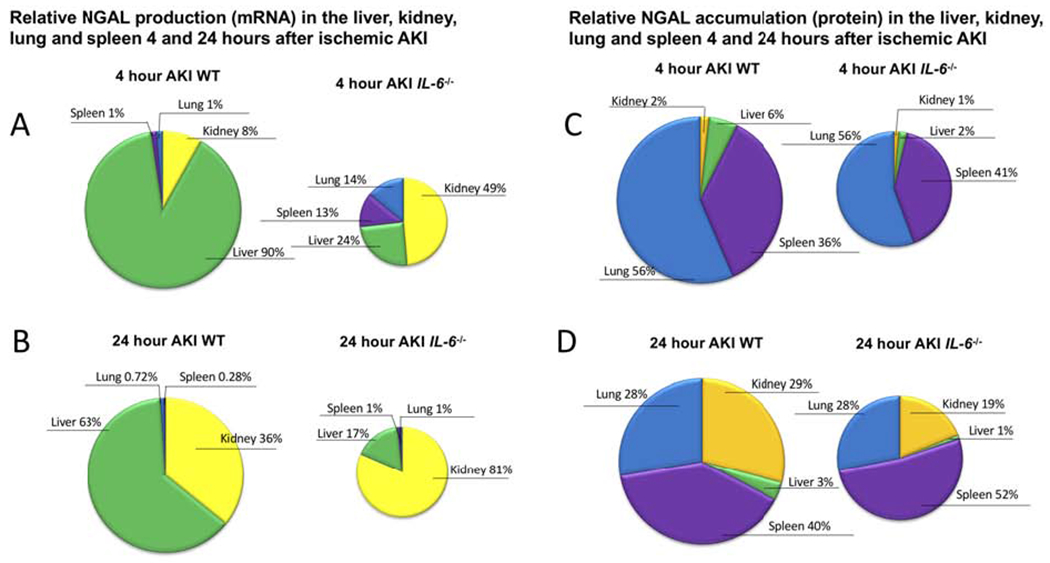
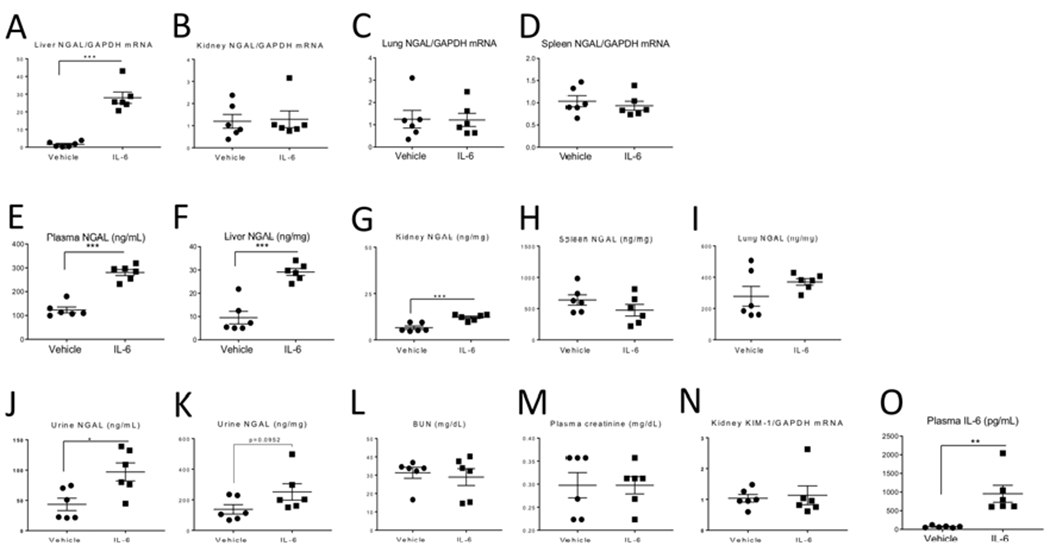
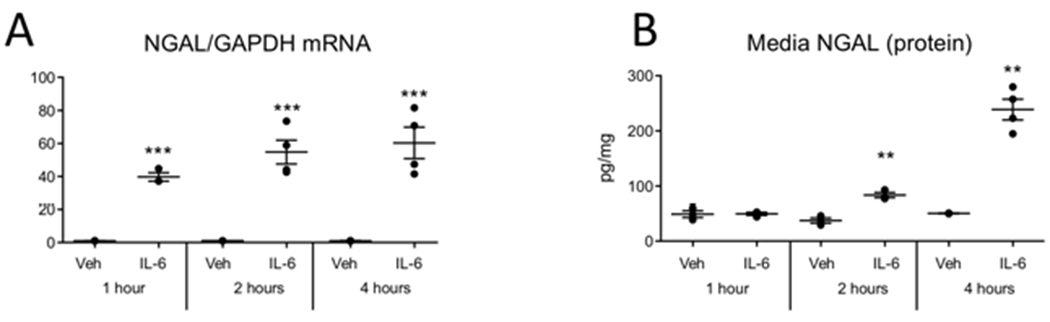
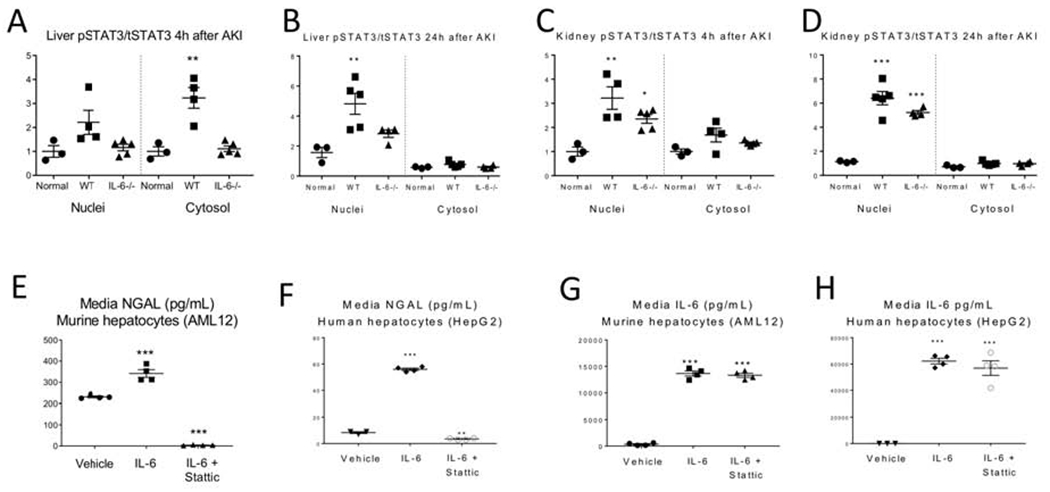
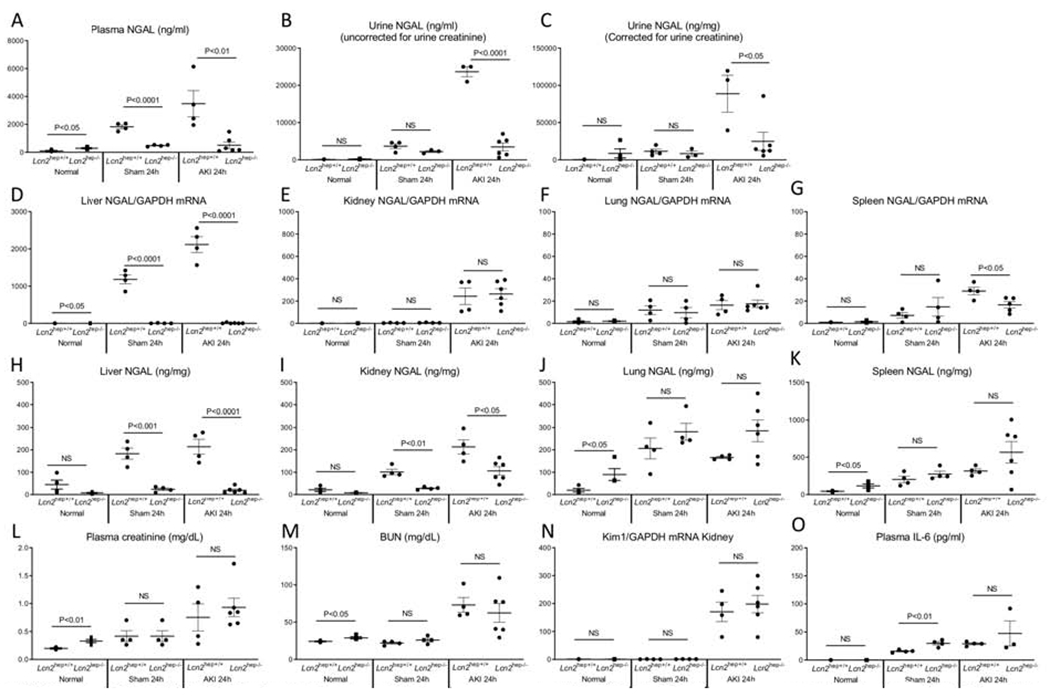
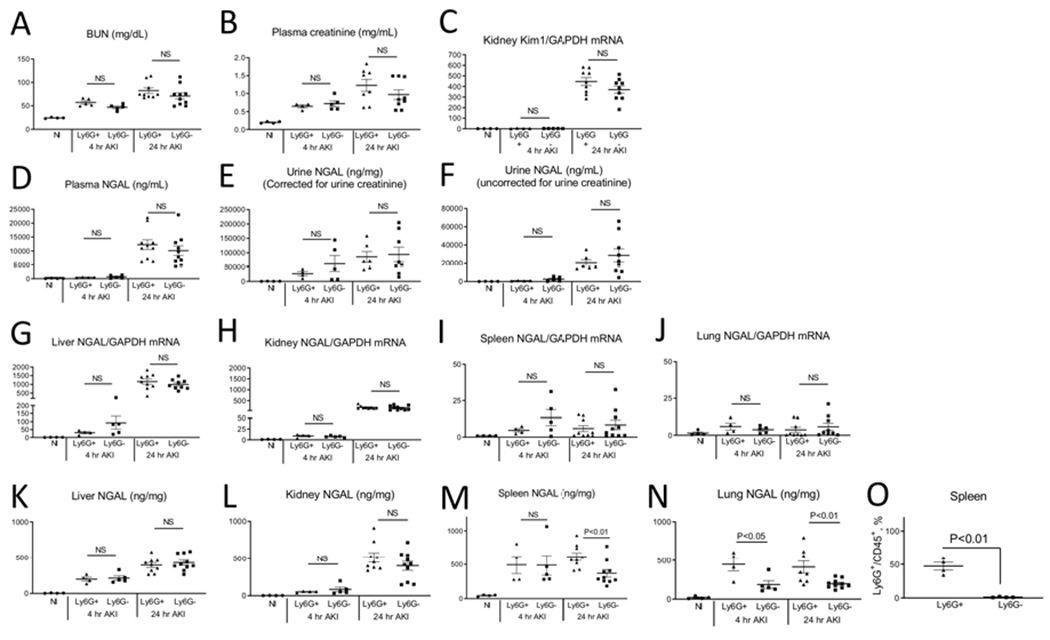
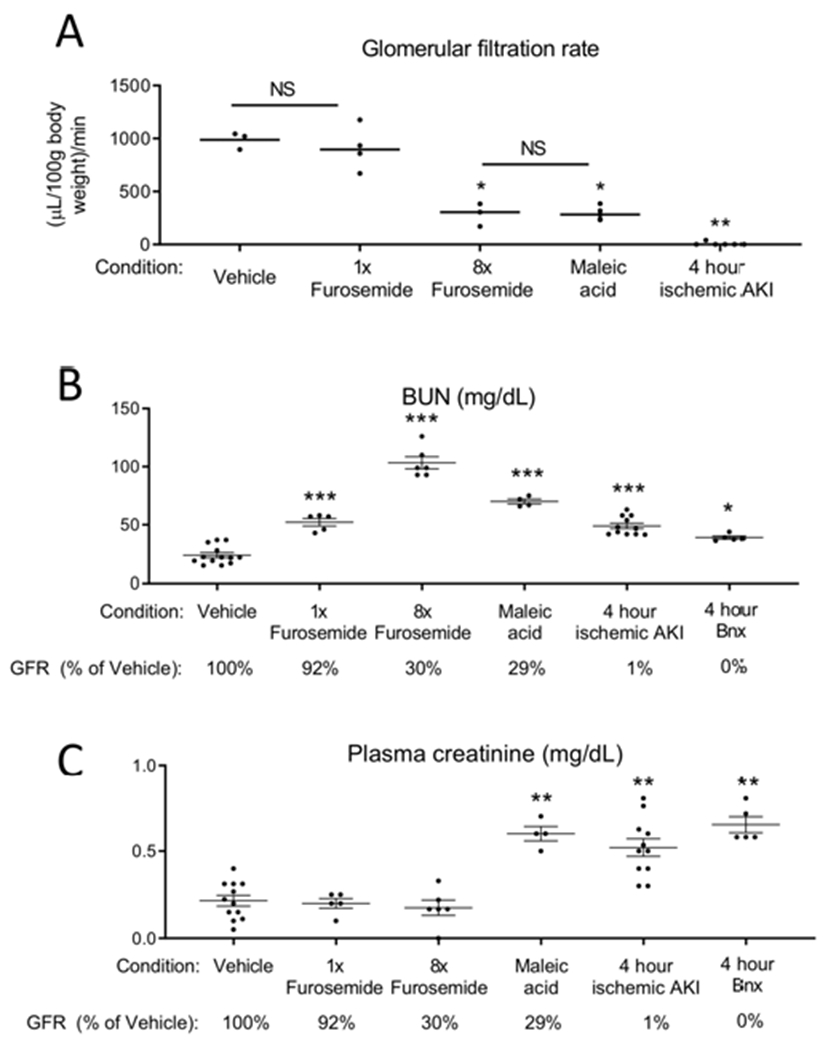
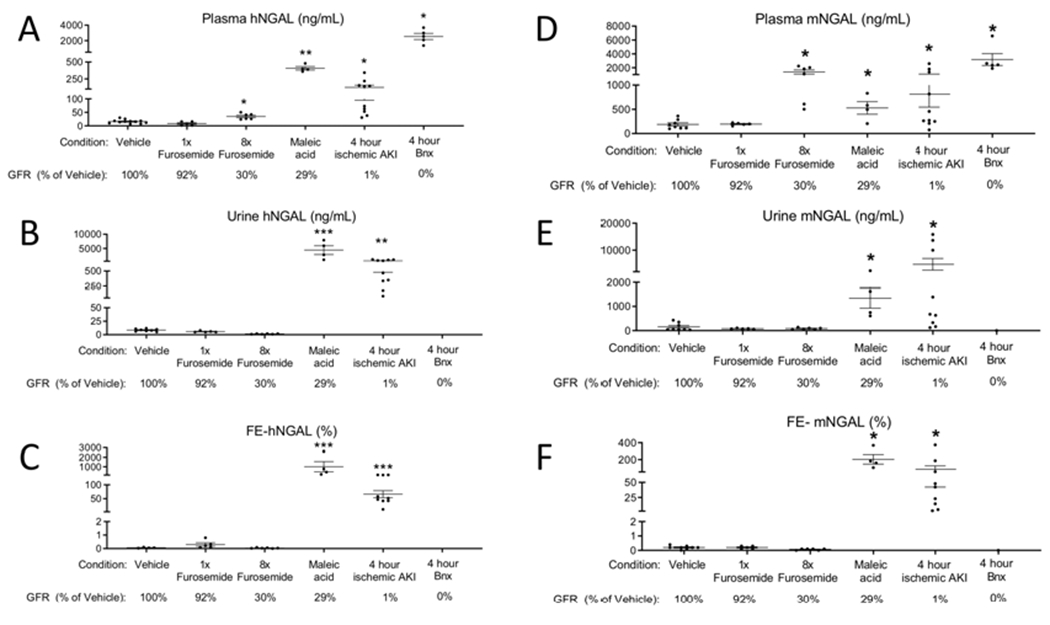
Neutrophil gelatinase associated lipocalin (NGAL, Lcn2) is the most widely studied biomarker of acute kidney injury (AKI). Previous studies have demonstrated that NGAL is produced by the kidney and released into the urine and plasma. Consequently, NGAL is currently considered a tubule specific injury marker of AKI. However, the utility of NGAL to predict AKI has been variable suggesting that other mechanisms of production are present. IL-6 is a proinflammatory cytokine increased in plasma by two hours of AKI and mediates distant organ effects. Herein, we investigated the role of IL-6 in renal and extra-renal NGAL production. Wild type mice with ischemic AKI had increased plasma IL-6, increased hepatic NGAL mRNA, increased plasma NGAL, and increased urine NGAL; all reduced in IL-6 knockout mice. Intravenous IL-6 in normal mice increased hepatic NGAL mRNA, plasma NGAL and urine NGAL. In mice with hepatocyte specific NGAL deletion (Lcn2hep-/-) and ischemic AKI, hepatic NGAL mRNA was absent, and plasma and urine NGAL were reduced. Since urine NGAL levels appear to be dependent on plasma levels, the renal handling of circulating NGAL was examined using recombinant human NGAL. After intravenous recombinant human NGAL administration to mice, human NGAL in mouse urine was detected by ELISA during proximal tubular dysfunction, but not in pre-renal azotemia. Thus, during AKI, IL-6 mediates hepatic NGAL production, hepatocytes are the primary source of plasma and urine NGAL, and plasma NGAL appears in the urine during proximal tubule dysfunction. Hence, our data change the paradigm by which NGAL should be interpreted as a biomarker of AKI.
Keywords: IL-6; acute kidney injury; biomarkers; cytokines; ischemia reperfusion; nephrotoxicity.
Copyright © 2019 International Society of Nephrology. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
AKI: an enlightening acronym with a shadow side.Kidney Int. 2020 Jun;97(6):1301. doi: 10.1016/j.kint.2020.03.016. Kidney Int. 2020. PMID: 32444096 No abstract available.
-
The author replies.Kidney Int. 2020 Jun;97(6):1301-1302. doi: 10.1016/j.kint.2020.03.017. Kidney Int. 2020. PMID: 32444098 No abstract available.
References
-
- American Society of Nephrology Renal Research Report. J Am Soc Nephrol 2005; 16: 1886–1903. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
