

Determinants of birth asphyxia among newborns in Ethiopia: A systematic review and meta-analysis
- PMID: 32082102
- PMCID: PMC7012503
Determinants of birth asphyxia among newborns in Ethiopia: A systematic review and meta-analysis
Abstract
Objective: The aim of this systematic review and meta-analysis was to estimate the pooled magnitude of birth asphyxia and its determinants in Ethiopia.
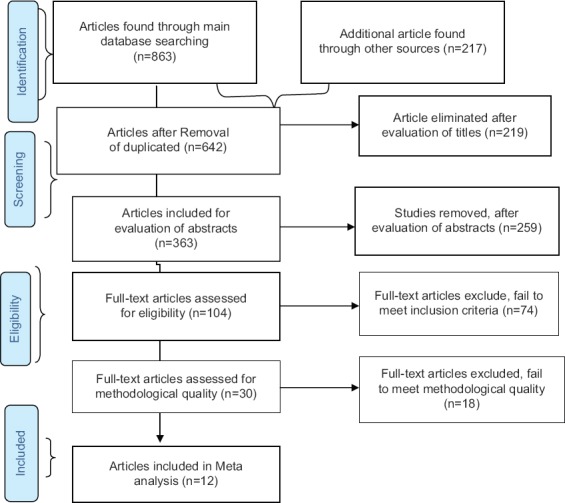
Methods: The databases, including PubMed, Medline, CINAHL, EMBASE, and other relevant sources, were used to search relevant articles. Both published and unpublished studies, written in English and carried out in Ethiopia, were included in the study. Quality of evidence was assessed by the relevant of the Joanna Briggs Institute tool. RevMan v5.3 statistical software was used to undertake the meta-analysis using a Mantel-Haenszel random-effects model. Heterogeneity was evaluated using the Cochran Q test, and I2 statistics was considered to assess its level. The outcome was measured using a 95% confidence interval (CI).
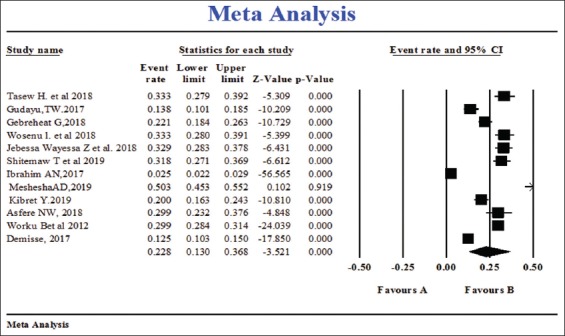
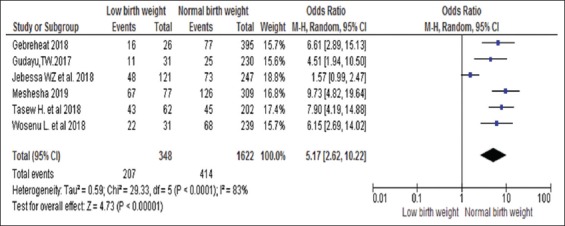
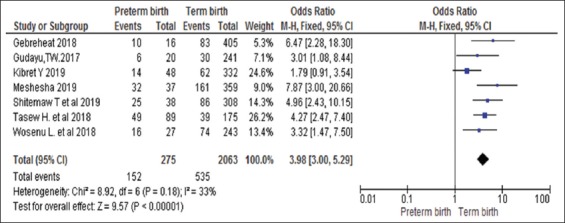
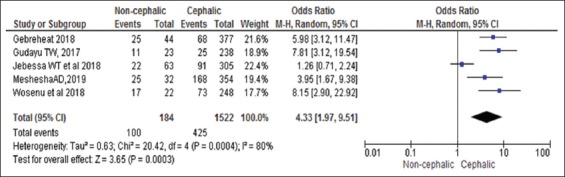
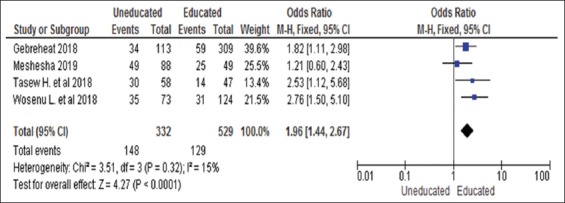
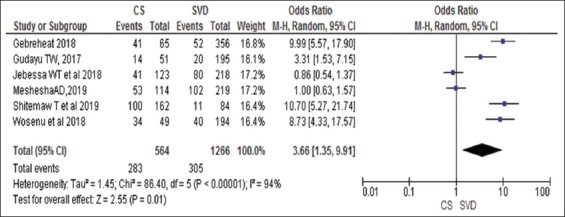
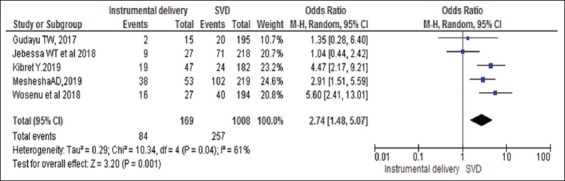
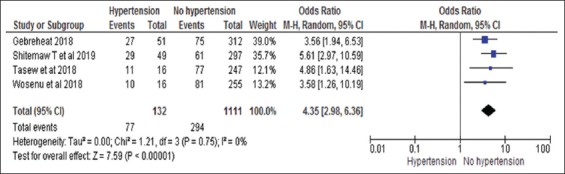
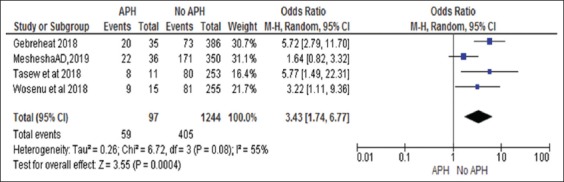
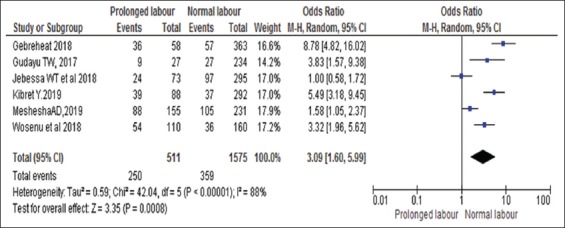
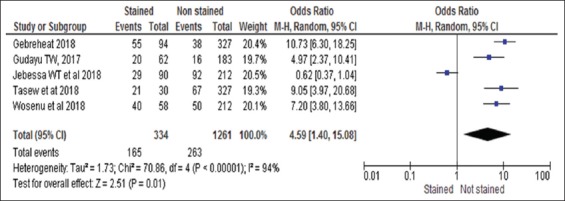
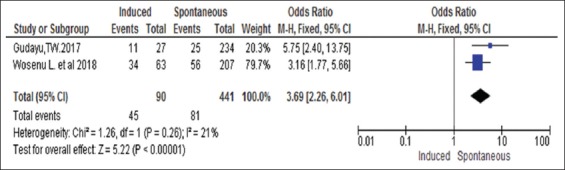
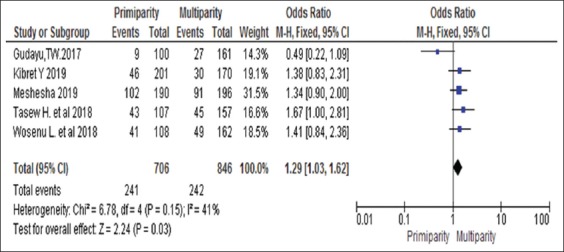
Results: The pooled prevalence of birth asphyxia was 22.8% (95% CI: 13-36.8%]. Illiterate mothers (adjusted odds ratio [AOR]; 1.96, 95% CI: 1.44-2.67), antepartum hemorrhage (APH) (AOR; 3.43, 95% CI: 1.74-6.77), cesarean section (AOR; 3.66, 95% CI: 1.35-9.91), instrumental delivery (AOR; 2.74, 95% CI: 1.48-5.08), duration of labor (AOR; 3.09, 95% CI: 1.60-5.99), pregnancy induced hypertension (AOR; 4.35, 95% CI: 2.98-6.36), induction of labor (AOR; 3.69, 95% CI: 2.26-6.01), parity (AOR; 1.29, 95% CI: 1.03-1.62), low birth weight (LBW) (AOR; 5.17, 95% CI: 2.62-10.22), preterm (AOR; 3.98, 95% CI: 3.00-5.29), non-cephalic presentation (AOR; 4.33, 95% CI: 1.97-9.51), and meconium staining (AOR; 4.59, 95% CI: 1.40-15.08) were significantly associated with birth asphyxia.
Conclusion: The magnitude of birth asphyxia was very high. Maternal education, APH, mode of delivery, prolonged labor, induction, LBW, preterm, meconium-staining, and non-cephalic presentation were determinants of birth asphyxia. Hence, to reduce birth asphyxia and associated neonatal mortality, attention should be directed to improve the quality of intrapartum service and timely communication between the delivery team. In addition, intervention strategies aimed at reducing birth asphyxia should target the identified determinants.
Keywords: Birth asphyxia; Ethiopia; determinant; newborn.
Copyright: © International Journal of Health Sciences.
Figures
References
-
- World Health Organization. Guidelines on Basic Newborn Resuscitation. Geneva: WHO Press; 2012. - PubMed
-
- Manu A, Arifeen S, Williams J, Mwasanya E, Zaka N, Plowman BA, et al. Assessment of facility readiness for implementing the WHO/UNICEF standards for improving quality of maternal and newborn care in health facilities experiences from UNICEF's implementation in three countries of South Asia and Sub-Saharan Africa. BMC Health Serv Res. 2018;18:531. - PMC - PubMed
-
- Ilah BG, Aminu MS, Musa A, Adelakun MB. Prevalence and risk factors for perinatal asphyxia as seen at a specialist hospital in Gusau, Nigeria. Sub-Saharan African J Med. 2015;2:1–6.
Publication types
LinkOut - more resources
Full Text Sources