

Results of late-onset type A aortic dissection after previous cardiac surgery: Does prior coronary artery bypass grafting affect survival?
- PMID: 32082704
- PMCID: PMC7018119
- DOI: 10.5606/tgkdc.dergisi.2018.14683
Results of late-onset type A aortic dissection after previous cardiac surgery: Does prior coronary artery bypass grafting affect survival?
Abstract
Background: This study aims to evaluate the results of late-onset type A aortic dissection following primary cardiac surgery and to compare the outcomes of patients with or without prior coronary artery bypass grafting.
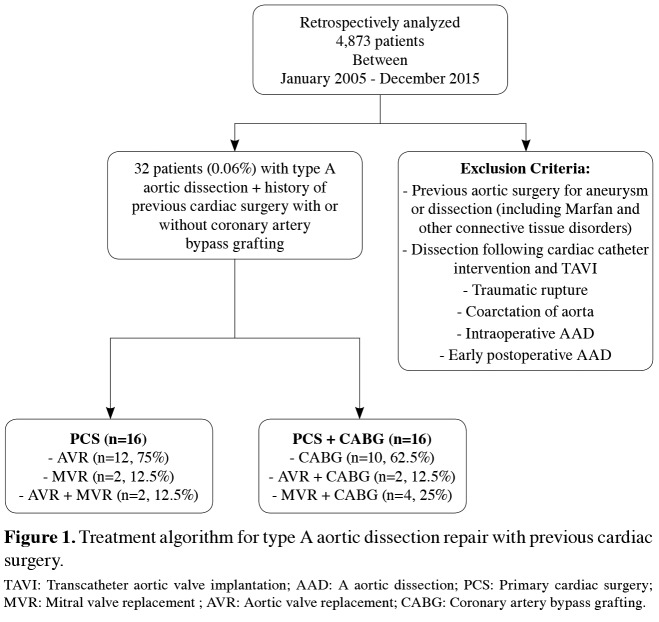
Methods: Between January 2005 and December 2015, data of 32 patients (16 males, 16 females; mean age 58.1±10.9 years; range, 45 to 73 years) who were diagnosed with acute type A aortic dissection and underwent repair with a history of previous cardiac surgery at our institution were retrospectively analyzed. The patients were divided into two groups as those with a history of prior coronary artery bypass grafting (n=16) and the patients with a previous cardiac surgery without prior coronary artery bypass grafting (n=16).
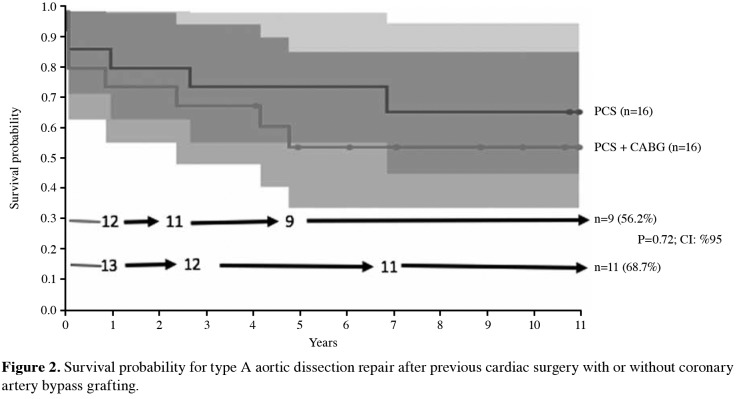
Results: Dissection of the ascending aorta occurred in 32 patients (late acute in 22 and late chronic in 10) who underwent previous cardiac surgery (aortic valve replacement in 12, mitral valve replacement in two, aortic valve replacement + coronary artery bypass grafting in two, coronary artery bypass grafting in 10, mitral valve replacement + coronary artery bypass grafting in four, and dual valve replacement in two patients). The mean time between the first operation and dissection was 4.0±1.5 years. Dissections were treated with the Bentall procedures (n=8), ascending aorta replacement (n=14), ascending aorta replacement + hemiarch replacement (n=4), ascending aorta + aortic valve replacement (n=4) and Bentall + arch replacement (n=2). In-hospital mortality (30-day mortality) was seen in five patients, and oneyear mortality rate was 21.85% (n=7). The survival rates of the all patients for primary cardiac surgery vs primary cardiac surgery + coronary artery bypass grafting were 81.25% vs 75% at one year, 75% vs 68.75% at three years,75% vs 56.25% at five years, 68.75% vs 56.25% at seven years, and 68.75% vs 56.25% at 10 years, respectively (p=0.71, CI: 95%).
Conclusion: Type-A aortic dissections may develop after cardiac operations with or without coronary artery bypass grafting at any time, and irrespective of associated histologies, they may result in high overall in-hospital mortality. With careful planning by prompt intervention, the outcomes in redo sternotomy operations with or without coronary artery bypass grafting for aortic dissections would be consistent the results of spontaneous aortic dissections.
Keywords: Aortic dissection; aortic surgery; cardiac valvular surgery.
Copyright © 2018, Turkish Society of Cardiovascular Surgery.
Conflict of interest statement
Conflict of Interest: The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Figures
References
-
- Salonen P, Rantanen A, Kellokumpu-Lehtinen PL, Huhtala H, Kaunonen M. The quality of life and social support in significant others of patients with breast cancer--a longitudinal study. Eur J Cancer Care (Engl) 2014;23:274–283. - PubMed
-
- LeMaire SA, Russell L. Epidemiology of thoracic aortic dissection. Nat Rev Cardiol. 2011;8:103–113. - PubMed
-
- Hiratzka LF, Bakris GL, Beckman JA, Bersin RM, Carr VF, Casey DE Jr, et al. 2010 ACCF/AHA/AATS/ ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: executive summary. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Catheter Cardiovasc Interv. 2010;76:43–86. - PubMed
-
- Collins JS, Evangelista A, Nienaber CA, Bossone E, Fang J, Cooper JV, et al. Differences in clinical presentation, management, and outcomes of acute type a aortic dissection in patients with and without previous cardiac surgery. Circulation. 2004;110:237–242. - PubMed
-
- Mehta RH, Suzuki T, Hagan PG, Bossone E, Gilon D, Llovet A, et al. Predicting death in patients with acute type a aortic dissection. Circulation. 2002;105:200–206. - PubMed
LinkOut - more resources
Full Text Sources