

Imaging for Metastasis in Prostate Cancer: A Review of the Literature
- PMID: 32083008
- PMCID: PMC7005012
- DOI: 10.3389/fonc.2020.00055
Imaging for Metastasis in Prostate Cancer: A Review of the Literature
Abstract
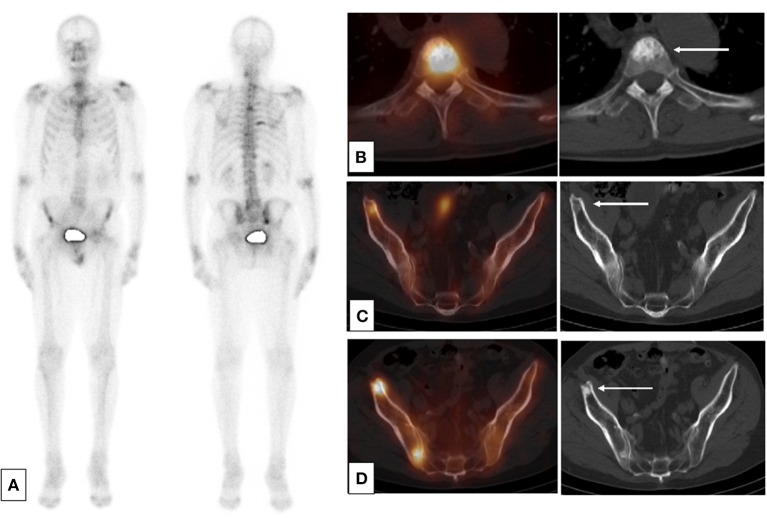
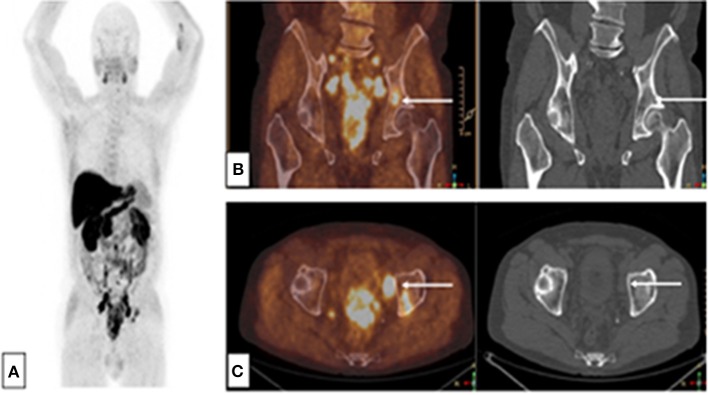
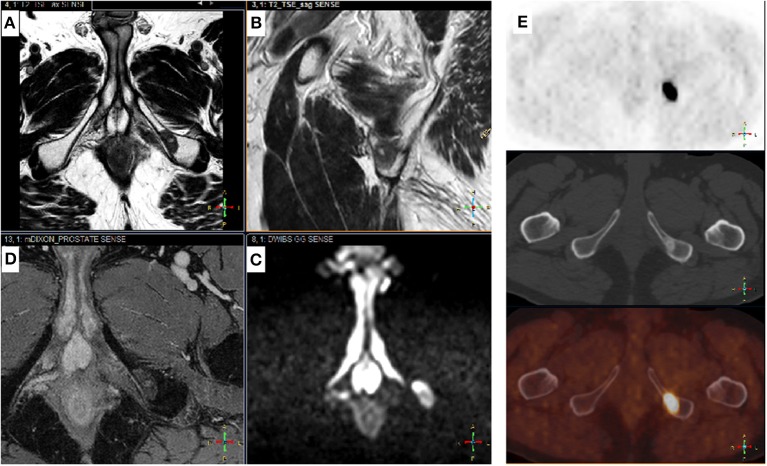
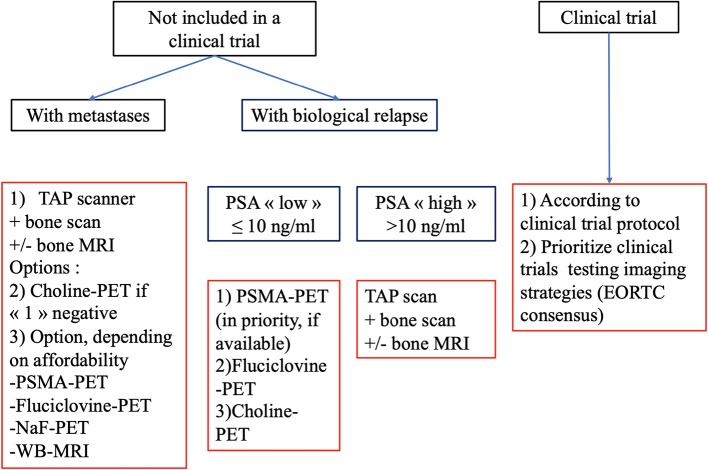
Background: Initial staging and assessment of treatment activity in metastatic prostate cancer (PCa) patients is controversial. Indications for the various available imaging modalities are not well-established due to rapid advancements in imaging and treatment. Methods: We conducted a critical literature review of the main imaging abnormalities that suggest a diagnosis of metastasis in localized and locally advanced PCa or in cases of biological relapse. We also assessed the role of the various imaging modalities available in routine clinical practice for the detection of metastases and response to treatment in metastatic PCa patients. Results: In published clinical trials, the most commonly used imaging modalities for the detection and evaluation of therapeutic response are bone scan, abdominopelvic computed tomography (CT), and pelvic and bone magnetic resonance imaging (MRI). For the detection and follow-up of metastases during treatment, modern imaging techniques i.e., choline-positron emission tomography (PET), fluciclovine-PET, or Prostate-specific membrane antigen (PSMA)-PET provide better sensitivity and specificity. This is particularly the case of fluciclovine-PET and PSMA-PET in cases of biochemical recurrence with low values of prostate specific antigen. Conclusions: In routine clinical practice, conventional imaging still have a role, and communication between imagers and clinicians should be encouraged. Present and future clinical trials should use modern imaging methods to clarify their usage.
Keywords: MRI; PSMA-PET; bone scan; choline-PET; fluciclovine-PET; prostate cancer; staging.
Copyright © 2020 Turpin, Girard, Baillet, Pasquier, Olivier, Villers, Puech and Penel.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous