

Growth Rates of Genetically Defined Renal Tumors: Implications for Active Surveillance and Intervention
- PMID: 32083993
- PMCID: PMC7145590
- DOI: 10.1200/JCO.19.02263
Growth Rates of Genetically Defined Renal Tumors: Implications for Active Surveillance and Intervention
Erratum in
-
Erratum.J Clin Oncol. 2021 Apr 10;39(11):1309. doi: 10.1200/JCO.21.00642. J Clin Oncol. 2021. PMID: 33826867 Free PMC article. No abstract available.
Abstract
Purpose: Published series of growth rates of renal tumors on active surveillance largely consist of tumors without pathologic or genetic data. Growth kinetics of genetically defined renal tumors are not well known. Here, we evaluate the growth of genetically defined renal tumors and their association with patient clinical and genetic characteristics.
Patients and methods: We evaluated patients with an inherited kidney cancer susceptibility syndrome as a result of a pathologic germline alteration of VHL, MET, FLCN, or BAP1 with at least 1 solid renal mass managed with active surveillance at our institution. Tumor growth rates (GR) were calculated and patients were stratified by genetic alteration and other clinical and genetic factors to analyze differences in growth rates using linear regression and comparative statistics.
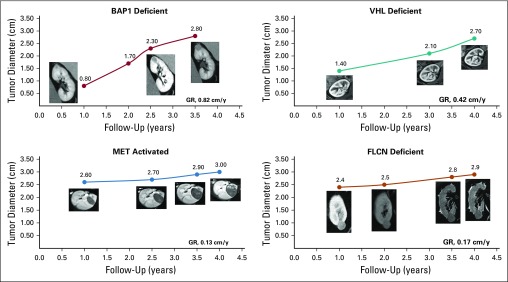
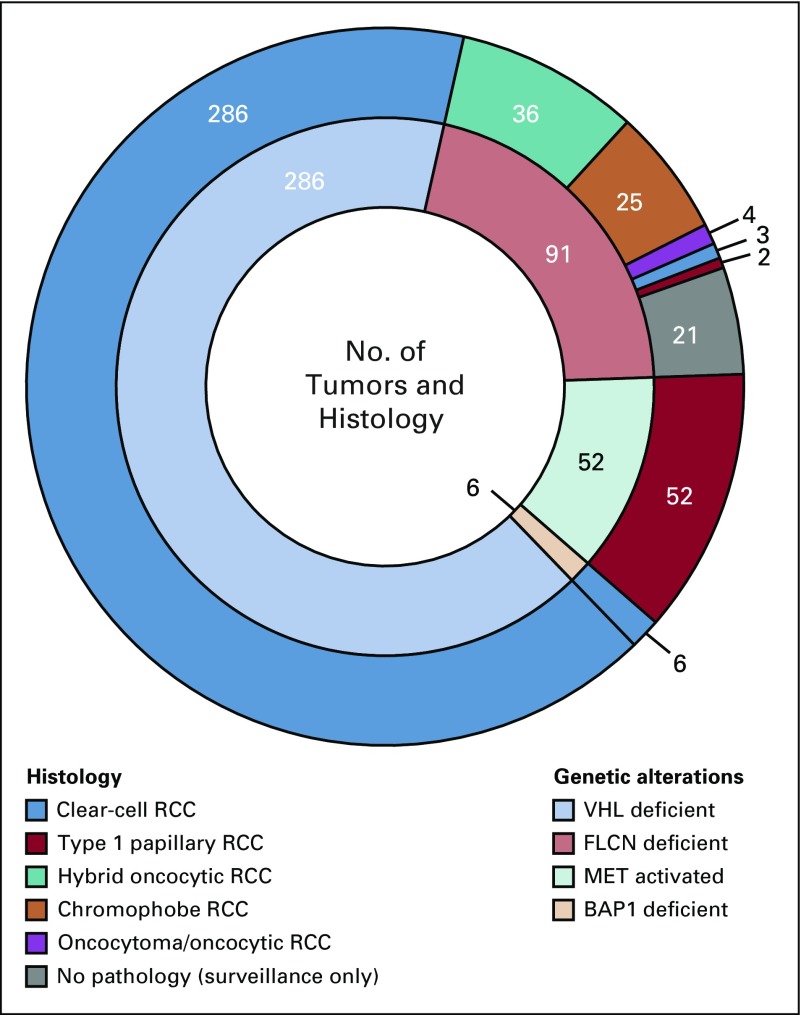
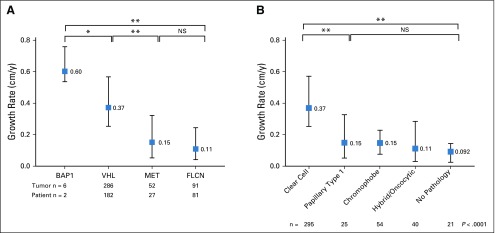
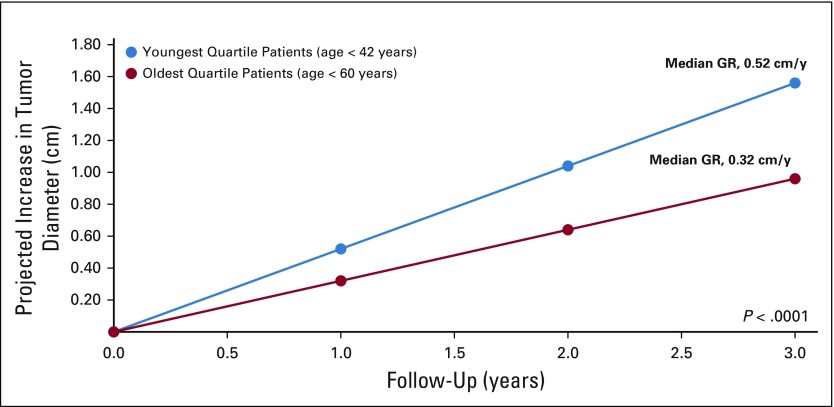
Results: A total of 292 patients with 435 genetically defined tumors were identified, including 286 VHL-deficient, 91 FLCN-deficient, 52 MET-activated, and 6 BAP1-deficient tumors. There were significant differences in GRs when stratified by genetic alteration. BAP1-deficient tumors had the fastest median GR (0.6 cm/y; interquartile range [IQR], 0.57-0.68 cm/y), followed by VHL-deficient tumors (GR, 0.37 cm/y; IQR, 0.25-0.57 cm/y), FLCN-deficient tumors (GR, 0.10 cm/y; IQR, 0.04-0.24 cm/y), and tumors with MET activation (GR, 0.15 cm/y; IQR, 0.053-0.32 cm/y; P < .001). Tumors from the same patient had similar GRs. Younger age was independently associated with higher GR (P = .005).
Conclusion: In a cohort of genetically defined tumors, tumor growth rates varied in a clinically and statistically different manner according to genetic subtype. Rapid growth of BAP1-deficient tumors indicates that these patients should be managed with caution. The faster growth of tumors in younger patients may support more frequent imaging, whereas the slower growth of other tumors may support extended surveillance beyond annual imaging in some instances.
Figures
References
-
- Campbell S, Uzzo RG, Allaf ME, et al. Renal mass and localized renal cancer: AUA guideline. J Urol. 2017;198:520–529. - PubMed
-
- Pierorazio PM, Johnson MH, Ball MW, et al. Five-year analysis of a multi-institutional prospective clinical trial of delayed intervention and surveillance for small renal masses: The DISSRM registry. Eur Urol. 2015;68:408–415. - PubMed
-
- Pavlovich CP, Grubb RL, III, Hurley K, et al. Evaluation and management of renal tumors in the Birt-Hogg-Dubé syndrome. J Urol. 2005;173:1482–1486. - PubMed
-
- Herring JC, Enquist EG, Chernoff A, et al. Parenchymal sparing surgery in patients with hereditary renal cell carcinoma: 10-year experience. J Urol. 2001;165:777–781. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
