

Genomic Landscape of Waldenström Macroglobulinemia and Its Impact on Treatment Strategies
- PMID: 32083995
- PMCID: PMC7351339
- DOI: 10.1200/JCO.19.02314
Genomic Landscape of Waldenström Macroglobulinemia and Its Impact on Treatment Strategies
Abstract
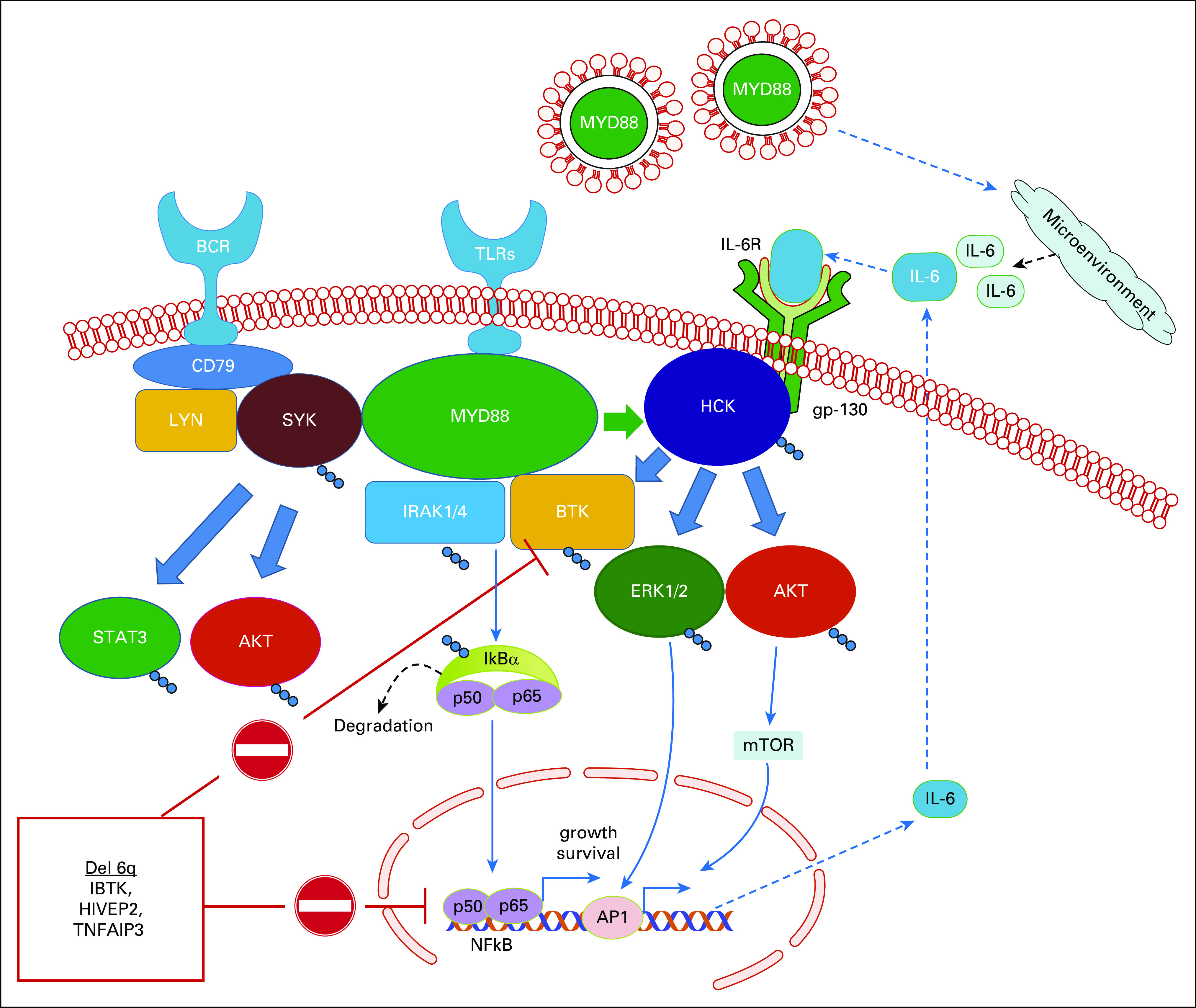
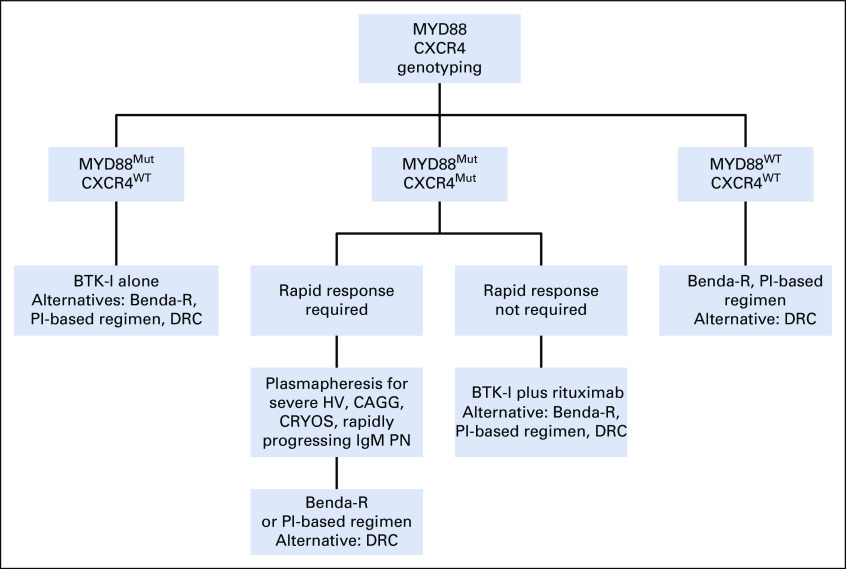
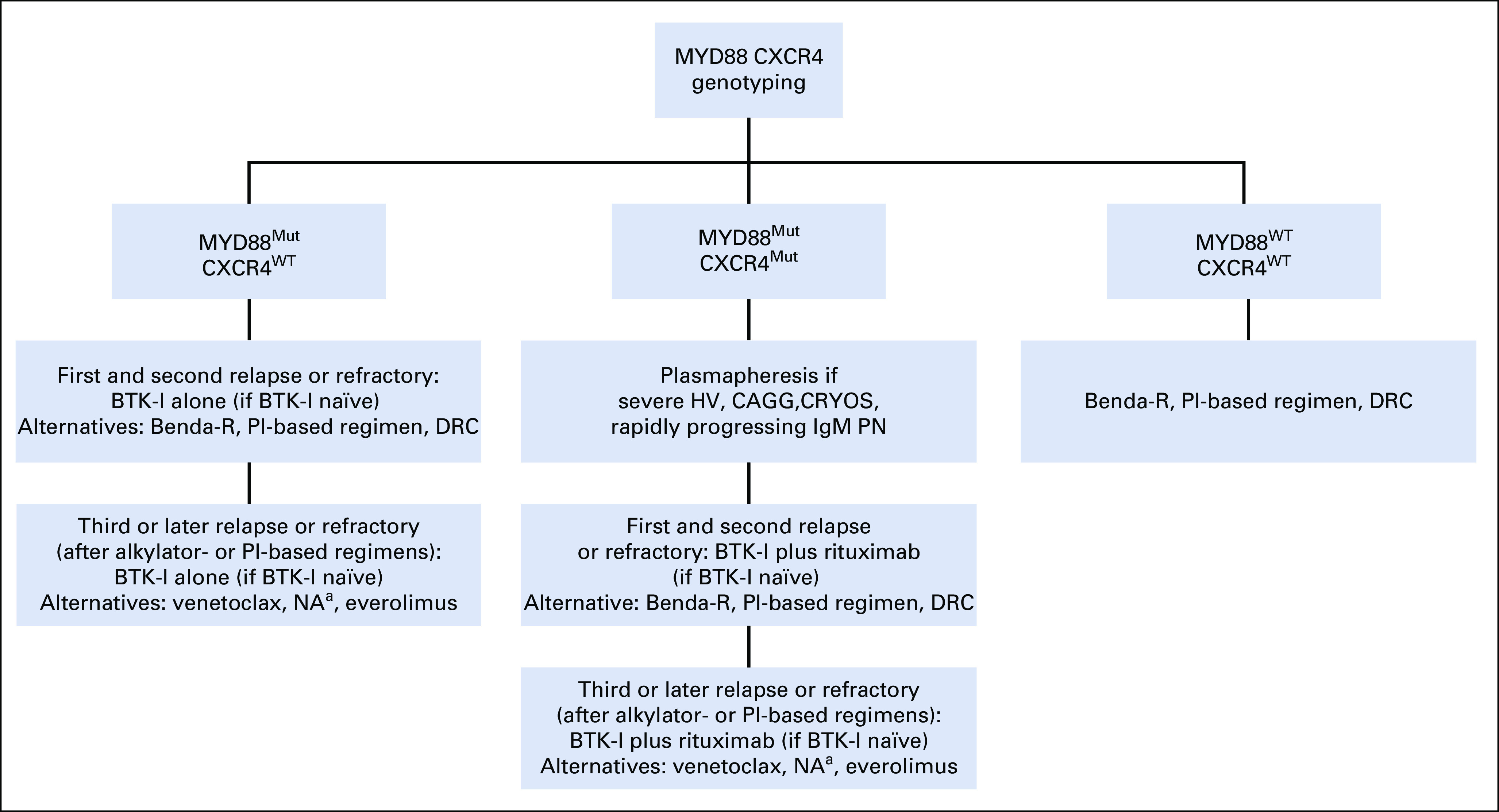
Next-generation sequencing has revealed recurring somatic mutations in Waldenström macroglobulinemia (WM), including MYD88 (95%-97%), CXCR4 (30%-40%), ARID1A (17%), and CD79B (8%-15%). Deletions involving chromosome 6q are common in patients with mutated MYD88 and include genes that modulate NFKB, BCL2, Bruton tyrosine kinase (BTK), and apoptosis. Patients with wild-type MYD88 WM show an increased risk of transformation and death and exhibit many mutations found in diffuse large B-cell lymphoma. The discovery of MYD88 and CXCR4 mutations in WM has facilitated rational drug development, including the development of BTK and CXCR4 inhibitors. Responses to many agents commonly used to treat WM, including the BTK inhibitor ibrutinib, are affected by MYD88 and/or CXCR4 mutation status. The mutation status of both MYD88 and CXCR4 can be used for a precision-guided treatment approach to WM.
Figures
References
-
- Treon SP. How I treat Waldenström macroglobulinemia. Blood. 2009;114:2375–2385. - PubMed
-
- Hunter ZR, Yang G, Xu L, et al. Genomics, signaling, and treatment of Waldenström macroglobulinemia. J Clin Oncol. 2017;35:994–1001. - PubMed
-
- Treon SP, Gustine J, Xu L, et al. MYD88 wild-type Waldenström macroglobulinaemia: Differential diagnosis, risk of histological transformation, and overall survival. Br J Haematol. 2018;180:374–380. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
