

Treatment-free interval as an additional measure of efficacy in a large UK dataset of transplant ineligible myeloma patients
- PMID: 32084254
- PMCID: PMC7034914
- DOI: 10.1371/journal.pone.0229469
Treatment-free interval as an additional measure of efficacy in a large UK dataset of transplant ineligible myeloma patients
Abstract
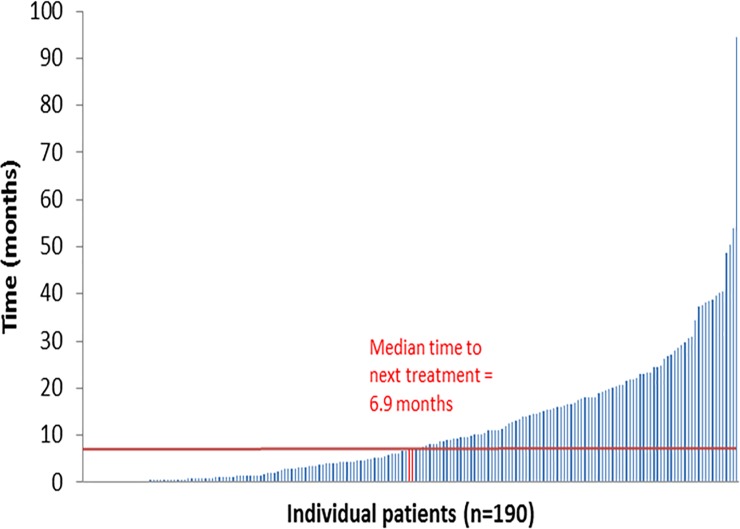
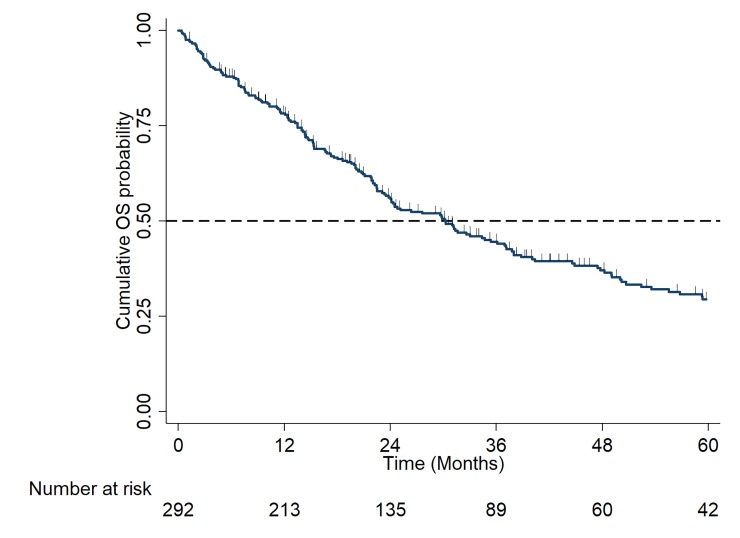
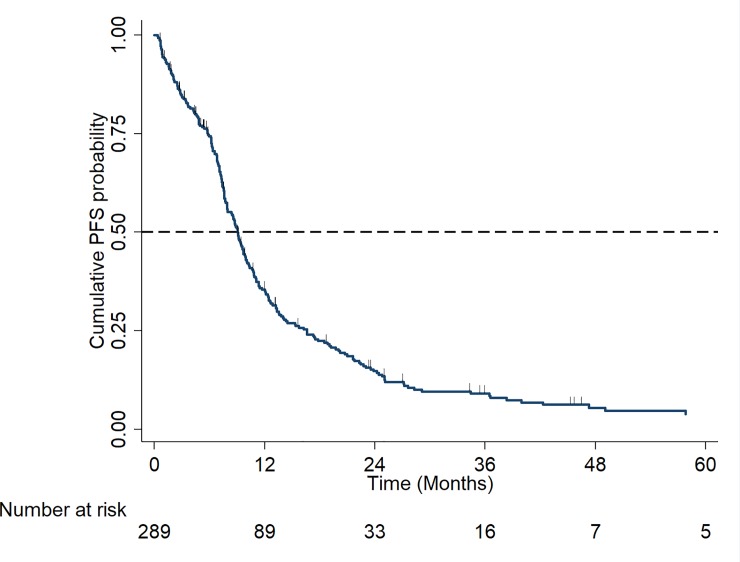
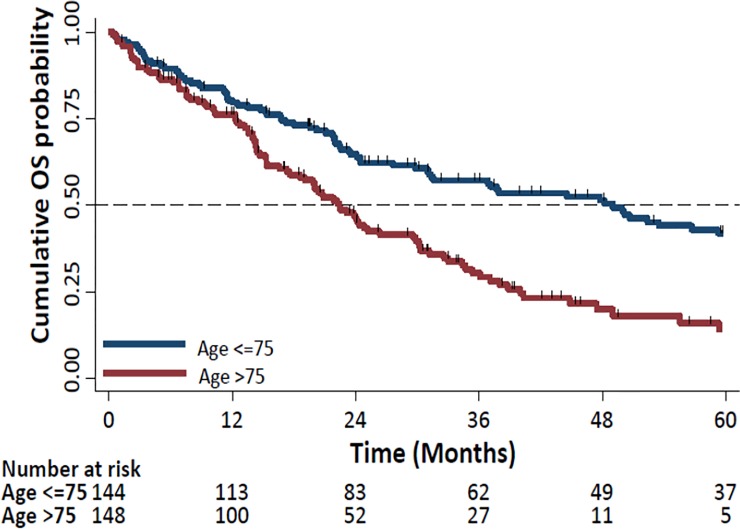
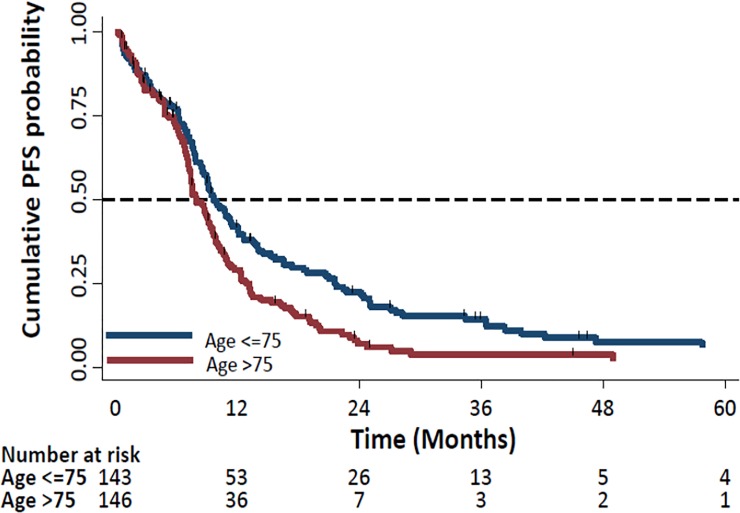
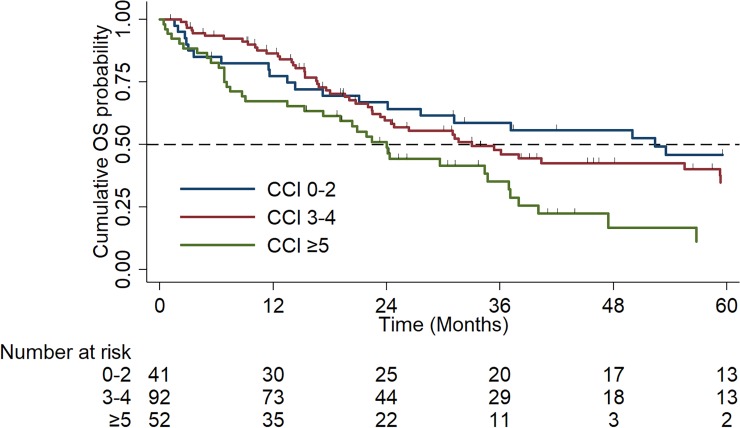
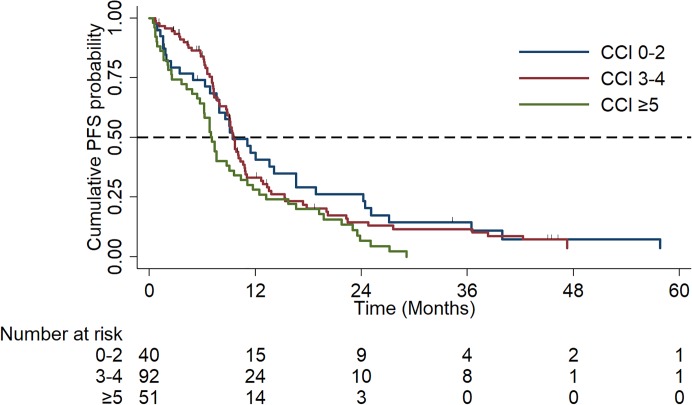
Treatment of transplant-ineligible (TNE) newly diagnosed multiple myeloma (NDMM) requires a balance between disease control and maintaining quality of life (QoL). Patients value treatment-free remission periods in this incurable condition, as they are associated with better QoL. We set out to study clinical outcomes of consecutive TNE NDMM patients in routine care treated in Thames Valley Cancer Network between 2009 and 2017. The primary outcome was the evaluation of the treatment-free interval (TFI) after 1st and subsequent lines of therapy in the total cohort and in individual subgroups, according to age (≤75 vs. >75 years), and co-morbidities using Charlson Co-morbidity Index (CCI): mild: 0-2 vs. moderate: 3-4 vs. severe: ≥5). Secondary outcomes include response rates, overall survival (OS) and progression-free survival (PFS) between subgroups: according to age and according to co-morbidities. In a total cohort of 292 patients, median TFI (IQR) was longest after first-line therapy 6.9 months (1.4-16.9), reducing after second line therapy to 1.8 months (.7-6.9), and after third line therapy to 0.6 months (0.2-1.5). Median TFI followed the same trend across the different subgroups, by age (≤75, >75 years) and by CCI (0-2, 3-4, ≥5). Overall response rate (ORR) to first line therapy for total cohort was 67%, with responses categorised as complete response (CR): 21%, very good partial response: 16%, partial response: 30%, stable disease: 18%, and progressive disease: 8%. ORR in individual subgroups by age were (≤75: 70% vs. >75: 63%), and by CCI (0-2: 65% vs. 3-4: 71% vs. ≥5: 77%). Median OS and PFS for the total cohort were (30.2 months, 95% CI: 23.8-36.9), and (9 months, 95% CI: 7.9-9.8), respectively. Patients aged >75 years showed a significant reduction in OS and PFS compared to those ≤75 years of age: OS (49.0 vs. 22.4 months, p<0.0001, HR: 2.08, 95% CI: 1.5-2.8), PFS (9.7 vs. 8.0 months, p<0.01, HR: 1.47, 95% CI: 1.1-1.9). Median OS was significantly reduced with worsening co-morbidities: (CCI 0-2: 52.4 months vs. CCI 3-4: 33.0 months vs. CCI ≥5: 24.0 months, p = 0.01, HR: 1.43, 95% CI: 1.1-1.9). Median PFS was significantly reduced in the severely co-morbid subgroup (CCI 0-2: 9.4 months vs. CCI 3-4: 9.6 months vs. CCI ≥5: 7.1 months, p = 0.025, HR: 1.3, 95% CI: 1.0-1.6). This study demonstrated that first line therapy in the TNE NDMM setting resulted in the longest TFI which was modest at a median of 6.9 months, and decreased significantly following subsequent lines of therapy and across the different subgroups by age and by co-morbidities. Therapy objective should be to maximise the benefit of first line treatment. We envisage that the recent shift towards a continuous therapeutic approach will benefit TNE patients in view of improved survival data demonstrated by a number phase 3 trials. When continuous therapy is not appropriate due to patient choice or toxicities, an efficacious (not limited to thalidomide and bortezomib) but tolerable first line FDT strategy, which can maximise TFI and maintain a good QoL, remains a reasonable alternative approach.
Conflict of interest statement
FD:Takeda:Honorarium, Travel to scientific conferences, Celgene: Honorarium, Research support, Travel to scientific conferences. Novartis: Honorarium, Amgen: Honorarium. FAS: Celgene: Educational Grant. SMS: employee of pH Associates and responsible for statistical analysis. GV: Nil. TAE: Nil. JK: Nil. SM: Nil. KR: Celgene: Honoraria, Research Grant; Janssen: Honoraria, Research Grant. None of the commercial affiliations described here alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Cancer Research UK. Cancer statistics: Myeloma incidence statistics. Available from: http://www.cancerresearchuk.org/health-professional/cancer-statistics/st.... Accessed April 4, 2018
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
