

Metabolic Reprogramming in Autosomal Dominant Polycystic Kidney Disease: Evidence and Therapeutic Potential
- PMID: 32086281
- PMCID: PMC7133124
- DOI: 10.2215/CJN.13291019
Metabolic Reprogramming in Autosomal Dominant Polycystic Kidney Disease: Evidence and Therapeutic Potential
Abstract
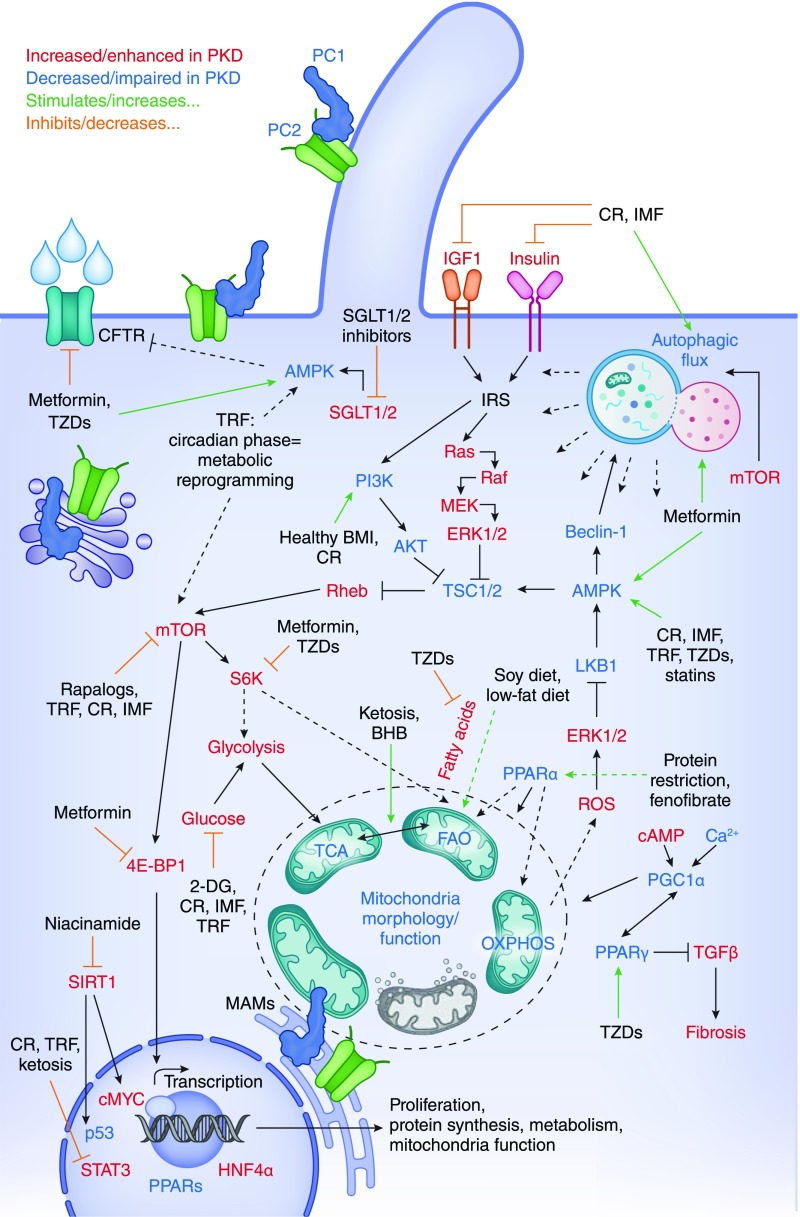
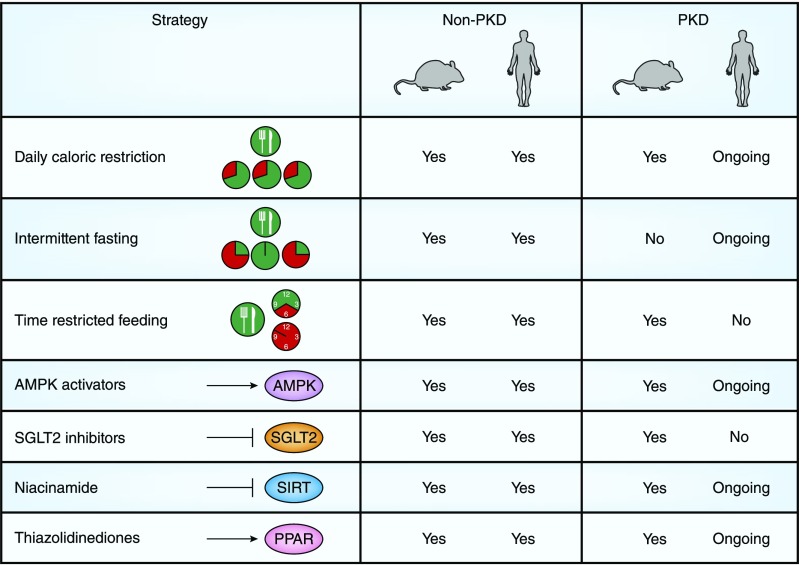
Autosomal dominant polycystic kidney disease is characterized by progressive development and enlargement of kidney cysts, leading to ESKD. Because the kidneys are under high metabolic demand, it is not surprising that mounting evidence suggests that a metabolic defect exists in in vitro and animal models of autosomal dominant polycystic kidney disease, which likely contributes to cystic epithelial proliferation and subsequent cyst growth. Alterations include defective glucose metabolism (reprogramming to favor aerobic glycolysis), dysregulated lipid and amino acid metabolism, impaired autophagy, and mitochondrial dysfunction. Limited evidence supports that cellular kidney metabolism is also dysregulated in humans with autosomal dominant polycystic kidney disease. There are notable overlapping features and pathways among metabolism, obesity, and/or autosomal dominant polycystic kidney disease. Both dietary and pharmacologic-based strategies targeting metabolic abnormalities are being considered as therapies to slow autosomal dominant polycystic kidney disease progression and are attractive, particularly given the slowly progressive nature of the disease. Dietary strategies include daily caloric restriction, intermittent fasting, time-restricted feeding, a ketogenic diet, and 2-deoxy-glucose as well as alterations to nutrient availability. Pharmacologic-based strategies include AMP-activated kinase activators, sodium glucose cotransporter-2 inhibitors, niacinamide, and thiazolidenediones. The results from initial clinical trials targeting metabolism are upcoming and anxiously awaited within the scientific and polycystic kidney disease communities. There continues to be a need for additional mechanistic studies to better understand the role of dysregulated metabolism in autosomal dominant polycystic kidney disease and for subsequent translation to clinical trials. Beyond single-intervention trials focused on metabolic reprograming in autosomal dominant polycystic kidney disease, great potential also exists by combining metabolic-focused therapeutic approaches with compounds targeting other signaling cascades altered in autosomal dominant polycystic kidney disease, such as tolvaptan.
Keywords: AMP-activated protein kinases; animal models; animals; autophagy; autosomal dominant polycystic kidney; caloric restriction; chronic kidney failure; cysts; deoxyglucose; diet; fasting; glucose; glycolysis; humans; ketogenic diet; kidney; lipids; metabolism; mitochondria; niacinamide; obesity; polycystic kidney disease; sodium-glucose transporter 2 inhibitors; tolvaptan; type 2 diabetes mellitus.
Copyright © 2020 by the American Society of Nephrology.
Figures
References
-
- Torres VE, Harris PC, Pirson Y: Autosomal dominant polycystic kidney disease. Lancet 369: 1287–1301, 2007 - PubMed
-
- Menezes LF, Germino GG: The pathobiology of polycystic kidney disease from a metabolic viewpoint. Nat Rev Nephrol 15: 735–749, 2019 - PubMed
-
- Padovano V, Podrini C, Boletta A, Caplan MJ: Metabolism and mitochondria in polycystic kidney disease research and therapy. Nat Rev Nephrol 14: 678–687, 2018 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
