

Real-world evidence on impact of a pharmacist-led transitional care program on 30- and 90-day readmissions after acute care episodes
- PMID: 32086512
- PMCID: PMC7090882
- DOI: 10.1093/ajhp/zxaa012
Real-world evidence on impact of a pharmacist-led transitional care program on 30- and 90-day readmissions after acute care episodes
Abstract
Purpose: Recent evidence suggests that improving the transitional care process may reduce 30-day readmissions and hospital length of stay (LOS). The objective of this study was to evaluate the impact of a pharmacist-led transitions-of-care (TOC) program on 30- and 90-day all-cause readmissions and LOS for patients discharged from the hospital acute care setting.
Methods: A retrospective cohort study was conducted using a difference-in-difference (DID) approach. Patients who were at least 18 years old with any of the following primary diagnoses were included: acute myocardial infarction, chronic obstructive pulmonary disease, congestive heart failure (CHF), and pneumonia. Outcome measures were all-cause 30- and 90-day readmission and LOS for the index admission.
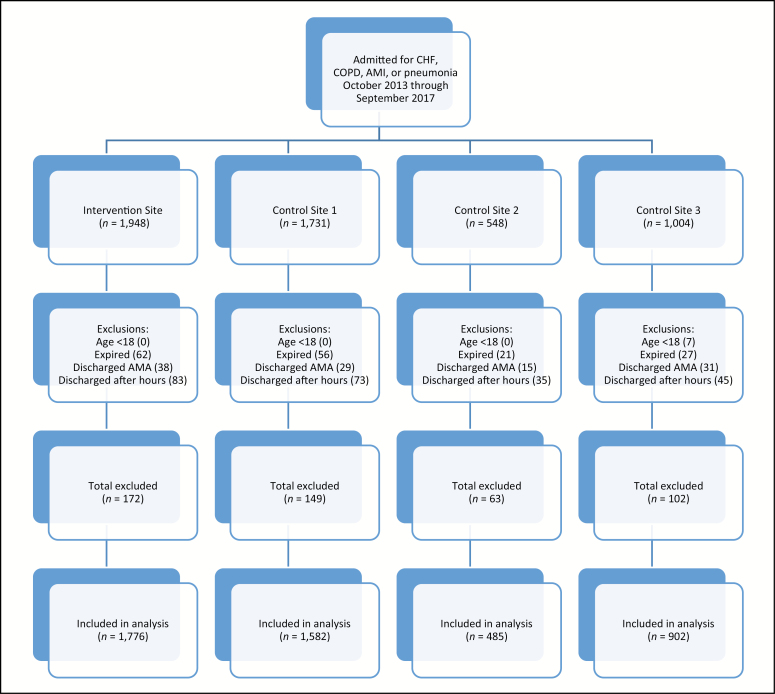
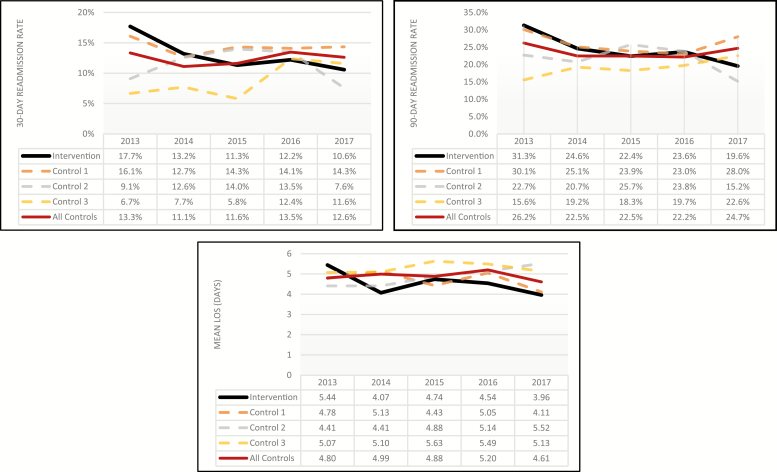
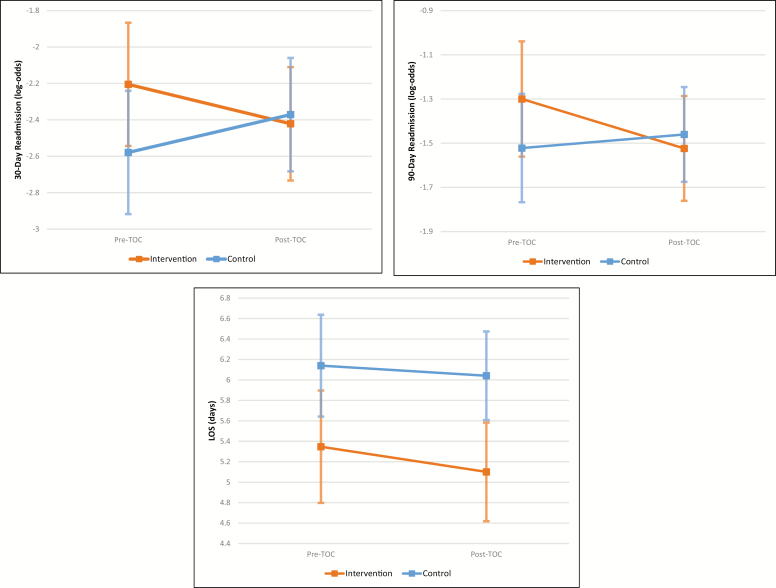
Results: From October 2013 through September 2017, 1,776 patients were discharged from the intervention site, and 2,969 patients were discharged from 3 control sites. Only 33.3% of eligible patients at the intervention site actually received the intervention. The DID analysis showed that the odds ratio (OR) for 30-day readmission was 0.65 [P = 0.035] at the intervention site following TOC program initiation. The OR for 90-day readmission was 0.75 [P = 0.070]. Among all diagnosis groups, the CHF subgroup had the highest proportion of patients who actually received the TOC intervention (57.2%). Within that CHF subgroup, the ORs for 30- and 90-day readmissions were 0.52 [P = 0.056] and 0.47 [P = 0.005], respectively. The mean LOS did not change significantly in either analysis.
Conclusion: This pharmacist-led transitional care intervention was associated with significantly decreased inpatient readmissions. The analysis indicates that pharmacist interventions can significantly reduce 30-day readmissions for high-risk populations and 90-day readmissions in patients with CHF.
Keywords: acute care; pharmacist-led services; readmissions; transition of care.
© American Society of Health-System Pharmacists 2020.
Figures
References
-
- A path to bundled payment around a rehospitalization. In: Report to the Congress: Reforming the Delivery System. Washington, DC: Medicare Payment Advisory Commission, June 2005:83-103.
-
- Burton R. Health policy brief: improving care transitions. Health Affairs.http://www.healthaffairs.org/healthpolicybriefs/brief.php?brief_id=76. Published September 2012. Accessed October 30, 2018.
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418-1428. - PubMed
-
- Centers for Medicare & Medicaid Services. Hospital Readmissions Reduction Program (HRRP).https://www.cms.gov/medicare/medicare-fee-for-service-payment/acuteinpat.... Accessed January 20, 2019.
