Outcomes after pneumonectomy versus limited lung resection in adults with traumatic lung injury
- PMID: 32086773
- PMCID: PMC7223758
- DOI: 10.1007/s13304-020-00727-4
Outcomes after pneumonectomy versus limited lung resection in adults with traumatic lung injury
Abstract
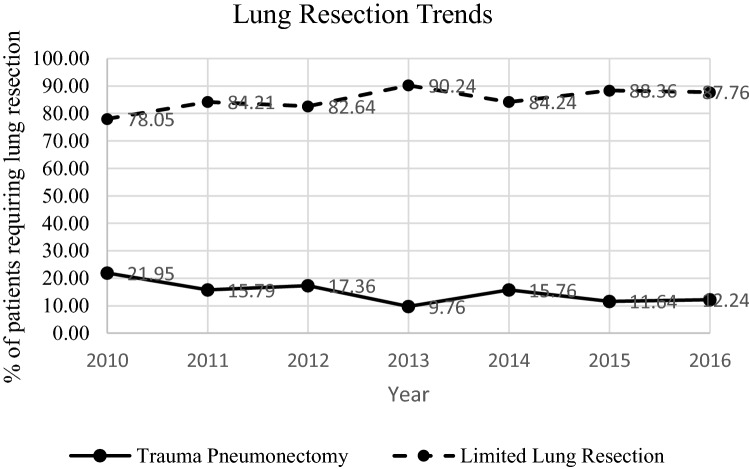
Pneumonectomy after traumatic lung injury (TLI) is associated with shock, increased pulmonary vascular resistance, and eventual right ventricular failure. Historically, trauma pneumonectomy (TP) mortality rates ranged between 53 and 100%. It is unclear if contemporary mortality rates have improved. Therefore, we evaluated outcomes associated with TP and limited lung resections (LLR) (i.e., lobectomy and segmentectomy) and aimed to identify predictors of mortality, hypothesizing that TP is associated with greater mortality versus LLR. We queried the Trauma Quality Improvement Program (2010-2016) and performed a multivariable logistic regression to determine the independent predictors of mortality in TLI patients undergoing TP versus LLR. TLI occurred in 287,276 patients. Of these, 889 required lung resection with 758 (85.3%) undergoing LLR and 131 (14.7%) undergoing TP. Patients undergoing TP had a higher median injury severity score (26.0 vs. 24.5, p = 0.03) but no difference in initial median systolic blood pressure (109 vs. 107 mmHg, p = 0.92) compared to LLR. Mortality was significantly higher for TP compared to LLR (64.9% vs 27.2%, p < 0.001). The strongest independent predictor for mortality was undergoing TP versus LLR (OR 4.89, CI 3.18-7.54, p < 0.001). TP continues to be associated with a higher mortality compared to LLR. Furthermore, TP is independently associated with a fivefold increased risk of mortality compared to LLR. Future investigations should focus on identifying parameters or treatment modalities that improve survivability after TP. We recommend that surgeons reserve TP as a last-resort management given the continued high morbidity and mortality associated with this procedure.
Keywords: Limited lung resections; Trauma pneumonectomy; Traumatic lung injury.
Conflict of interest statement
The authors report no conflicts of interest, financial or otherwise.
Figures