

Paravertebral catheter versus EPidural analgesia in Minimally invasive Esophageal resectioN: a randomized controlled multicenter trial (PEPMEN trial)
- PMID: 32087686
- PMCID: PMC7036230
- DOI: 10.1186/s12885-020-6585-1
Paravertebral catheter versus EPidural analgesia in Minimally invasive Esophageal resectioN: a randomized controlled multicenter trial (PEPMEN trial)
Abstract
Background: Thoracic epidural analgesia is the standard postoperative pain management strategy in esophageal cancer surgery. However, paravertebral block analgesia may achieve comparable pain control while inducing less side effects, which may be beneficial for postoperative recovery. This study primarily aims to compare the postoperative quality of recovery between paravertebral catheter versus thoracic epidural analgesia in patients undergoing minimally invasive esophagectomy.
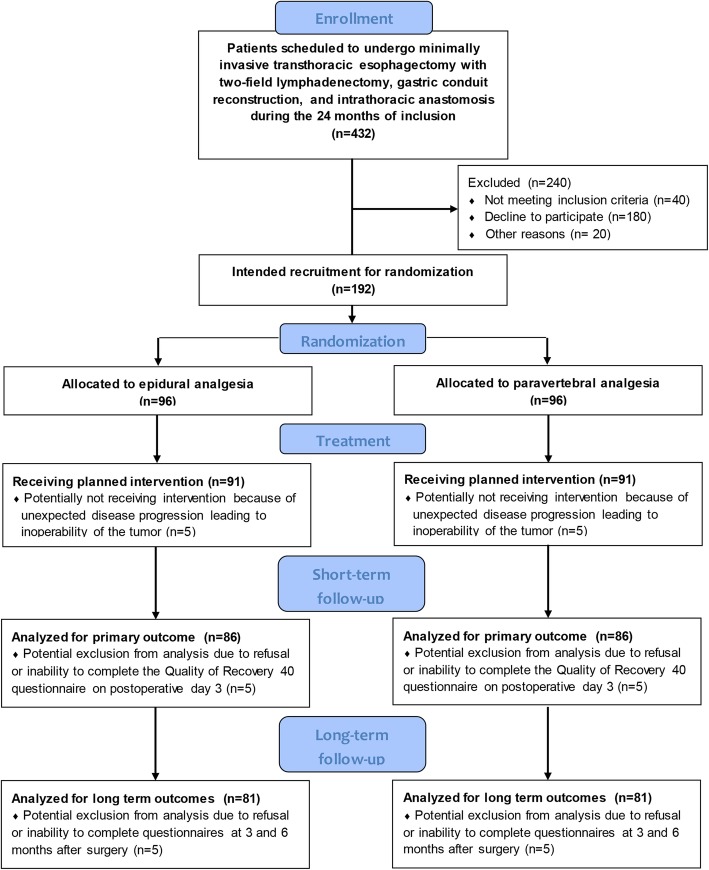
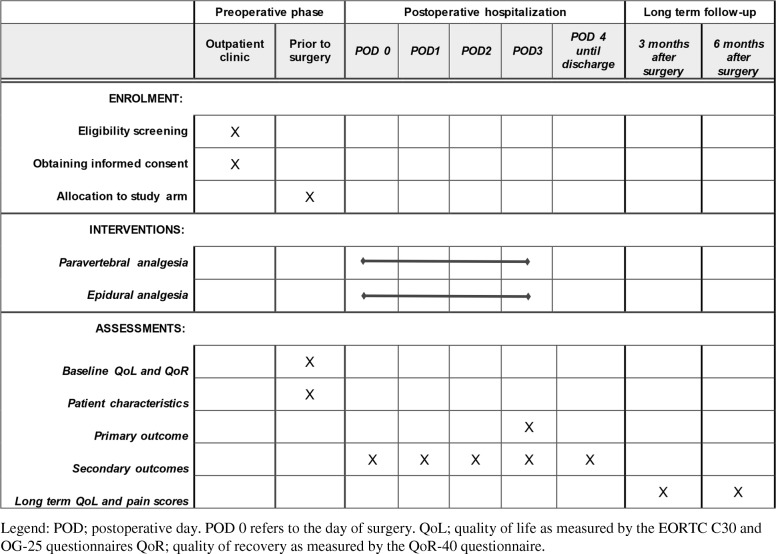
Methods: This study represents a randomized controlled superiority trial. A total of 192 patients will be randomized in 4 Dutch high-volume centers for esophageal cancer surgery. Patients are eligible for inclusion if they are at least 18 years old, able to provide written informed consent and complete questionnaires in Dutch, scheduled to undergo minimally invasive esophagectomy with two-field lymphadenectomy and an intrathoracic anastomosis, and have no contra-indications to either epidural or paravertebral analgesia. The primary outcome is the quality of postoperative recovery, as measured by the Quality of Recovery-40 (QoR-40) questionnaire on the morning of postoperative day 3. Secondary outcomes include the QoR-40 questionnaire score Area Under the Curve on postoperative days 1-3, the integrated pain and systemic opioid score and patient satisfaction and pain experience according to the International Pain Outcomes (IPO) questionnaire, and cost-effectiveness. Furthermore, the groups will be compared regarding the need for additional rescue medication on postoperative days 0-3, technical failure of the pain treatment, duration of anesthesia, duration of surgery, total postoperative fluid administration day 0-3, postoperative vasopressor and inotrope use, length of urinary catheter use, length of hospital stay, postoperative complications, chronic pain at six months after surgery, and other adverse effects.
Discussion: In this study, it is hypothesized that paravertebral analgesia achieves comparable pain control while causing less side-effects such as hypotension when compared to epidural analgesia, leading to shorter postoperative length of stay on a monitored ward and superior quality of recovery. If this hypothesis is confirmed, the results of this study can be used to update the relevant guidelines on postoperative pain management for patients undergoing minimally invasive esophagectomy.
Trial registration: Netherlands Trial Registry, NL8037. Registered 19 September 2019.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Paravertebral Versus EPidural Analgesia in Minimally Invasive Esophageal ResectioN (PEPMEN): A Randomized Controlled Multicenter Trial.Ann Surg. 2025 Jul 1;282(1):29-36. doi: 10.1097/SLA.0000000000006551. Epub 2024 Oct 3. Ann Surg. 2025. PMID: 39360422 Free PMC article. Clinical Trial.
-
Ultrasound-guided erector spinae plane catheter versus video-assisted paravertebral catheter placement in minimally invasive thoracic surgery: comparing continuous infusion analgesic techniques on early quality of recovery, respiratory function and chronic persistent surgical pain: study protocol for a double-blinded randomised controlled trial.Trials. 2021 Dec 28;22(1):965. doi: 10.1186/s13063-021-05863-9. Trials. 2021. PMID: 34963493 Free PMC article.
-
Optimal postoperative pain management after VATS lung resection by thoracic epidural analgesia, continuous paravertebral block or single-shot intercostal nerve block (OPtriAL): study protocol of a three-arm multicentre randomised controlled trial.BMC Surg. 2022 Sep 4;22(1):330. doi: 10.1186/s12893-022-01765-y. BMC Surg. 2022. PMID: 36058900 Free PMC article.
-
Paravertebral anaesthesia with or without sedation versus general anaesthesia for women undergoing breast cancer surgery.Cochrane Database Syst Rev. 2021 Feb 25;2(2):CD012968. doi: 10.1002/14651858.CD012968.pub2. Cochrane Database Syst Rev. 2021. PMID: 33629404 Free PMC article.
-
Epidural anesthesia in esophagectomy: a systematic review and meta-analysis.J Gastrointest Surg. 2025 Jul;29(7):102093. doi: 10.1016/j.gassur.2025.102093. Epub 2025 May 21. J Gastrointest Surg. 2025. PMID: 40409490
Cited by
-
Efficacy and safety of Extrapleural block in patients with coronary artery disease after thoracoscopic surgery.Ann Noninvasive Electrocardiol. 2023 May;28(3):e13050. doi: 10.1111/anec.13050. Epub 2023 Feb 6. Ann Noninvasive Electrocardiol. 2023. PMID: 36745525 Free PMC article.
-
Association of Upper Gastrointestinal Surgery of Great Britain and Ireland (AUGIS)/Perioperative Quality Initiative (POQI) consensus statement on intraoperative and postoperative interventions to reduce pulmonary complications after oesophagectomy.Br J Surg. 2022 Oct 14;109(11):1096-1106. doi: 10.1093/bjs/znac193. Br J Surg. 2022. PMID: 36001582 Free PMC article.
-
Analgesic efficacy of surgeon placed paravertebral catheters compared with thoracic epidural analgesia after Ivor Lewis esophagectomy: a retrospective non-inferiority study.J Thorac Dis. 2024 Jan 30;16(1):414-422. doi: 10.21037/jtd-23-689. Epub 2024 Jan 18. J Thorac Dis. 2024. PMID: 38410611 Free PMC article.
-
Analgesia in esophagectomy: a narrative review.J Thorac Dis. 2023 Sep 28;15(9):5099-5111. doi: 10.21037/jtd-23-241. Epub 2023 Sep 1. J Thorac Dis. 2023. PMID: 37868851 Free PMC article. Review.
-
Feasibility and effectiveness of multi-injection thoracic paravertebral block via the intrathoracic approach for analgesia after thoracoscopic-laparoscopic esophagectomy.Esophagus. 2021 Jul;18(3):513-521. doi: 10.1007/s10388-020-00807-9. Epub 2021 Jan 6. Esophagus. 2021. PMID: 33403428 Free PMC article. Clinical Trial.
References
-
- Shapiro J, van Lanschot JJB, Hulshof MCCM, van Hagen P, van Berge Henegouwen MI, Wijnhoven BPL, et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial. Lancet Oncol. 2015;16(9):1090–1098. doi: 10.1016/S1470-2045(15)00040-6. - DOI - PubMed
-
- van der Sluis PC, Ruurda JP, Verhage RJ, van der Horst S, Haverkamp L, Siersema PD, et al. Oncologic long-term results of robot-assisted minimally invasive Thoraco-laparoscopic Esophagectomy with two-field lymphadenectomy for esophageal Cancer. Ann Surg Oncol. 2015;22(Suppl 3):S1350–S1356. doi: 10.1245/s10434-015-4544-x. - DOI - PMC - PubMed
-
- Richardson J, Sabanathan S, Mearns AJ, Evans CS, Bembridge J, Fairbrass M. Efficacy of pre-emptive analgesia and continuous extrapleural intercostal nerve block on post-thoracotomy pain and pulmonary mechanics. J Cardiovasc Surg. 1994;35(3):219–228. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
