

Cell-free DNA analysis reveals POLR1D-mediated resistance to bevacizumab in colorectal cancer
- PMID: 32087735
- PMCID: PMC7036260
- DOI: 10.1186/s13073-020-0719-6
Cell-free DNA analysis reveals POLR1D-mediated resistance to bevacizumab in colorectal cancer
Abstract
Background: Bevacizumab, a monoclonal antibody against soluble VEGFA, is an approved and commonly administered anti-angiogenic drug in patients with metastasized colorectal cancer (mCRC). The survival benefit of anti-VEGF therapy in mCRC patients is limited to a few months, and acquired resistance mechanisms are largely unknown. Here, we employed whole-genome sequencing of plasma DNA to evaluate the tumor genome of patients undergoing treatment with bevacizumab to determine novel aberrations associated with resistance.
Methods: Using longitudinal plasma analyses, we studied the evolution of tumor genomes in a mCRC cohort (n = 150) and conducted analyses of CRC cases from The Cancer Genome Atlas (TCGA) database (n = 619) to identify associations between genomic aberrations and clinical features. We employed whole-genome sequencing to identify the most frequently occurring focal somatic copy number alterations (SCNAs). Using the TCGA data as a comparative and supporting dataset, we defined the minimally amplified overlapping region and studied the mechanistic consequences of copy number gain of the involved genes in this segment. In addition, we established an in vitro cell model and conducted downstream gene expression and cell viability assays to confirm our findings from the patient dataset.
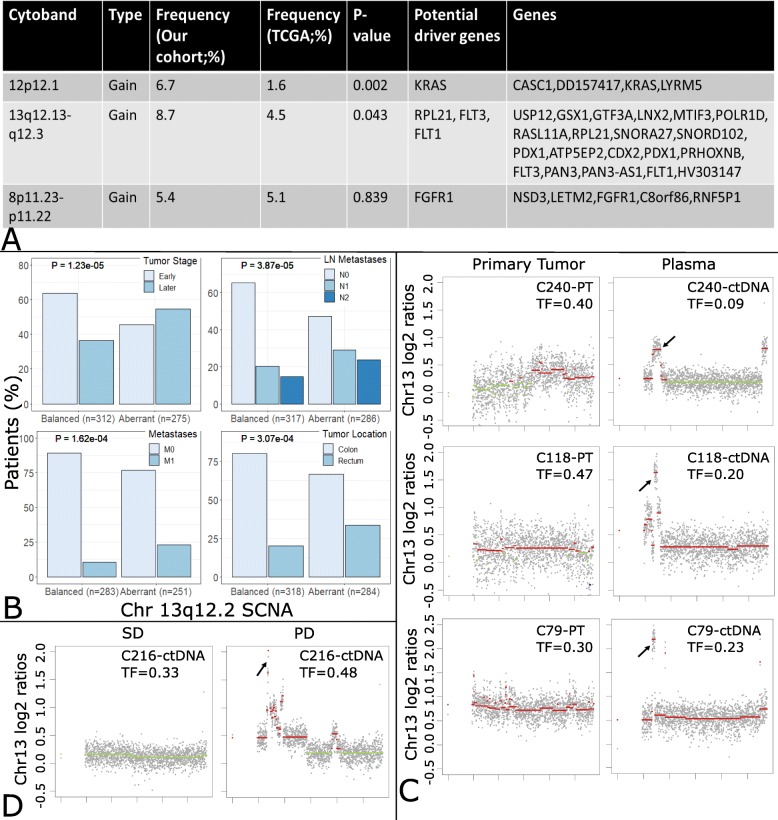
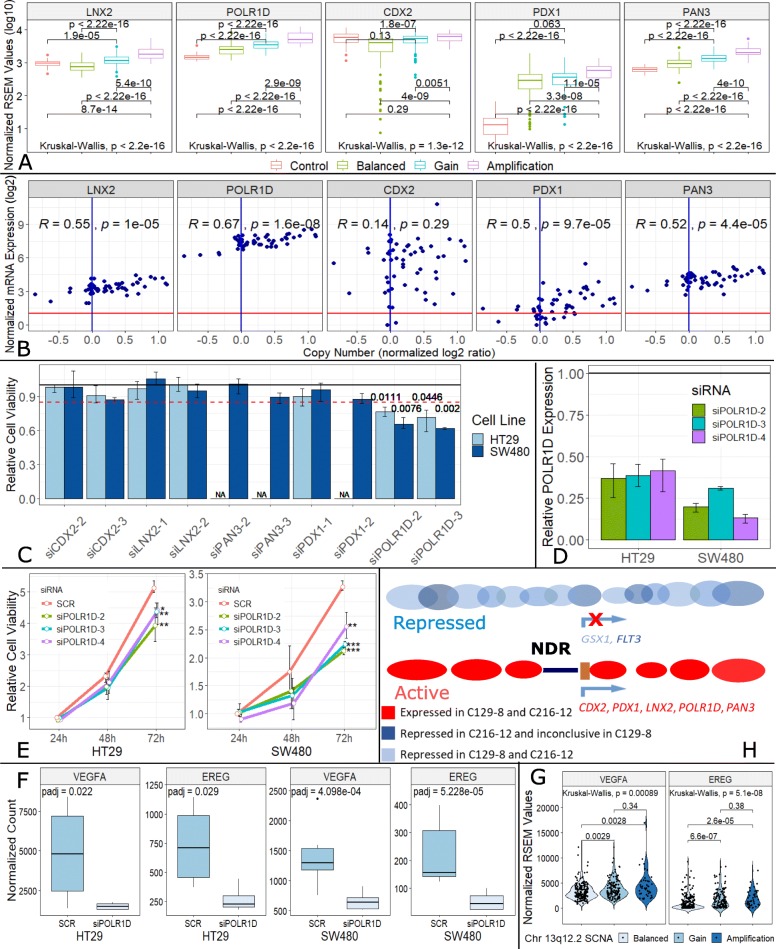
Results: We observed a recurrent focal amplification (8.7% of cases) on chromosome 13q12.2. Analysis of CRC cases from the TCGA database suggested that this amplicon is associated with more advanced stages. We confirmed that this 13q12.2 amplicon frequently emerges later during the clinical course of disease. After defining the minimally amplified region, we observed that the amplification and expression of one gene, POLR1D, impacted cell proliferation and resulted in upregulation of VEGFA, an important regulator of angiogenesis which has been implicated in the resistance to bevacizumab treatment. In fact, in several patients, we observed the emergence of this 13q12.2 amplicon under bevacizumab treatment, which was invariably associated with therapy resistance.
Conclusions: Non-invasive analyses of cell-free DNA from patients undergoing treatment with bevacizumab enabled the tracking of evolving tumor genomes and helped identify a recurrent focal SCNA of clinical relevance. Here, we describe a novel resistance mechanism against a widely applied treatment in patients with mCRC which will impact the clinical management of patients.
Keywords: Bevacizumab; Cell-free DNA; POLR1D; Precision medicine; Therapy resistance; Whole-genome sequencing.
Conflict of interest statement
PU is employed by Freenome. The remaining authors declare that they have no competing interests.
Figures



References
-
- Reissfelder C, Timke C, Schmitz-Winnenthal H, Rahbari NN, Koch M, Klug F, et al. A randomized controlled trial to investigate the influence of low dose radiotherapy on immune stimulatory effects in liver metastases of colorectal cancer. BMC Cancer. 2011;11:419–2407. doi: 10.1186/1471-2407-11-419. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
