

Investigating lupus retention in care to inform interventions for disparities reduction: an observational cohort study
- PMID: 32087763
- PMCID: PMC7036188
- DOI: 10.1186/s13075-020-2123-4
Investigating lupus retention in care to inform interventions for disparities reduction: an observational cohort study
Abstract
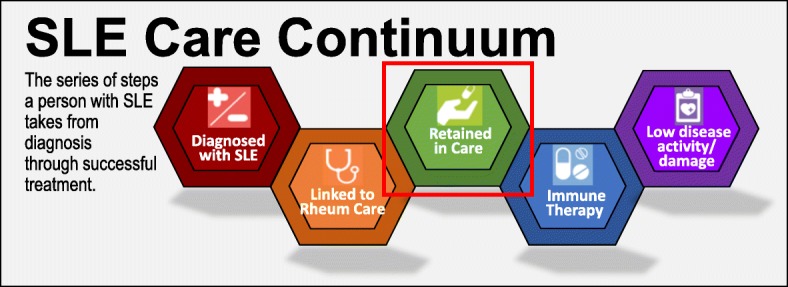
Background: Systemic lupus erythematous (SLE) disproportionately impacts patients of color and socioeconomically disadvantaged patients. Similar disparities in HIV were reduced through a World Health Organization-endorsed Care Continuum strategy targeting "retention in care," defined as having at least two annual visits or viral load lab tests. Using similar definitions, this study aimed to examine predictors of lupus retention in care, to develop an SLE Care Continuum and inform interventions to reduce disparities. We hypothesized that Black patients and those residing in disadvantaged neighborhoods would have lower retention in care.
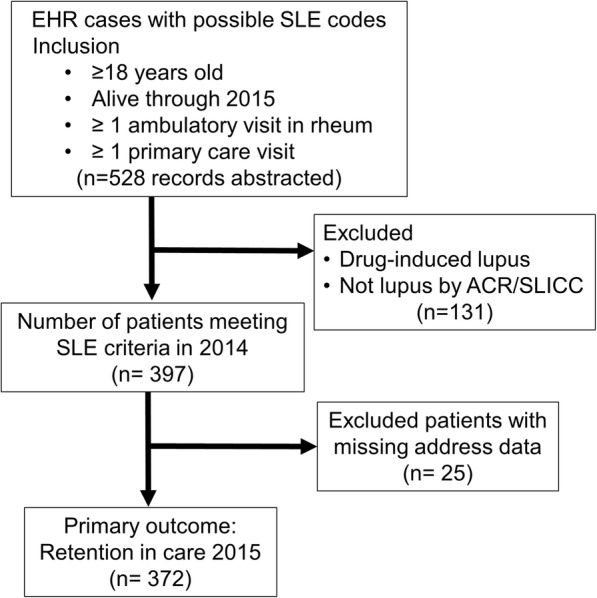
Methods: Abstractors manually validated 545 potential adult cases with SLE codes in 2013-2014 using 1997 American College of Rheumatology (ACR) or 2012 Systemic Lupus Erythematosus International Collaborating Clinics (SLICC) criteria. We identified 397 SLE patients who met ACR or SLICC criteria for definite lupus, had at least one baseline rheumatology visit, and were alive through 2015. Retention in care was defined as having two ambulatory rheumatology visits or SLE labs (e.g., complement tests) during the outcome year 2015, analogous to HIV retention definitions. Explanatory variables included age, sex, race, ethnicity, smoking status, neighborhood area deprivation index (ADI), number of SLE criteria, and nephritis. We used multivariable logistic regression to test our hypothesis and model predictors of SLE retention in care.
Results: Among 397 SLE patients, 91% were female, 56% White, 39% Black, and 5% Hispanic. Notably, 51% of Black versus 5% of White SLE patients resided in the most disadvantaged ADI neighborhood quartile. Overall, 60% met visit-defined retention and 27% met complement lab-defined retention in 2015. Retention was 59% lower for patients in the most disadvantaged neighborhood quartile (adjusted OR 0.41, CI 0.18, 0.93). No statistical difference was seen based on age, sex, race, or ethnicity. More SLE criteria and non-smoking predicted greater retention.
Conclusions: Disadvantaged neighborhood residence was the strongest factor predicting poor SLE retention in care. Future interventions could geo-target disadvantaged neighborhoods and design retention programs with vulnerable populations to improve retention in care and reduce SLE outcome disparities.
Keywords: Health care quality; Health disparities; Retention in care; Social determinants of health; Systemic lupus erythematosus.
Conflict of interest statement
CMB receives peer-reviewed institutional grant funding from the Independent Grants for Learning and Change (Pfizer) for research unrelated to this study. All other authors declare that they have no competing interests.
Figures
References
-
- U.S. Department of Health and Human Services, National Institutes of Health, National Institute of Arthritis and Musculoskeletal and Skin Diseases. The future directions of lupus research. Bethesda; 2007. https://www.niams.nih.gov/about/future-directions-lupus-research. Accessed 30 Sept 2019
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
