

Genetic Risk Underlying Psychiatric and Cognitive Symptoms in Huntington's Disease
- PMID: 32087949
- PMCID: PMC7156911
- DOI: 10.1016/j.biopsych.2019.12.010
Genetic Risk Underlying Psychiatric and Cognitive Symptoms in Huntington's Disease
Abstract
Background: Huntington's disease (HD) is an inherited neurodegenerative disorder caused by an expanded CAG repeat in the HTT gene. It is diagnosed following a standardized examination of motor control and often presents with cognitive decline and psychiatric symptoms. Recent studies have detected genetic loci modifying the age at onset of motor symptoms in HD, but genetic factors influencing cognitive and psychiatric presentations are unknown.
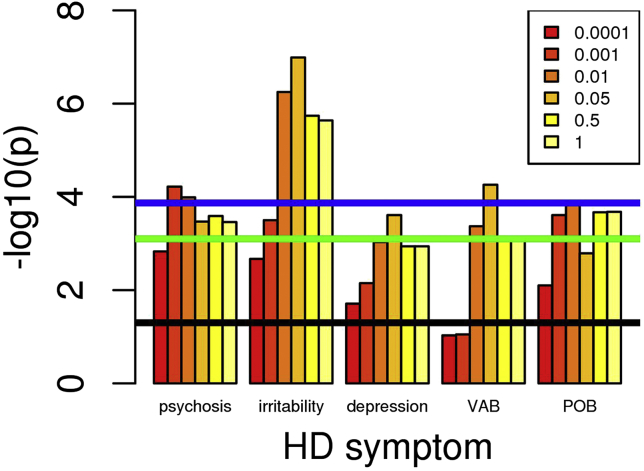
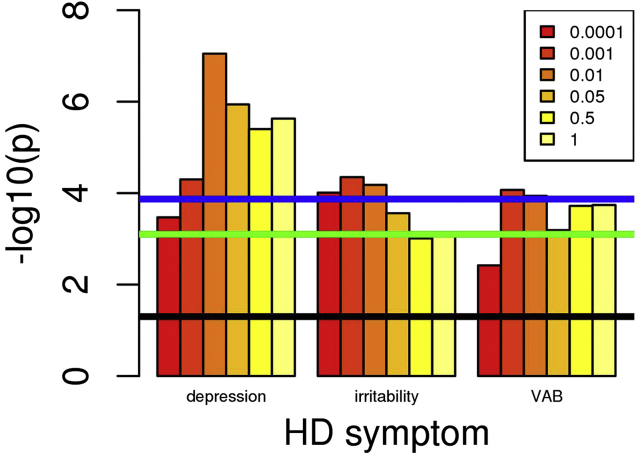
Methods: We tested the hypothesis that psychiatric and cognitive symptoms in HD are influenced by the same common genetic variation as in the general population by 1) constructing polygenic risk scores from large genome-wide association studies of psychiatric and neurodegenerative disorders and of intelligence and 2) testing for correlation with the presence of psychiatric and cognitive symptoms in a large sample (n = 5160) of patients with HD.
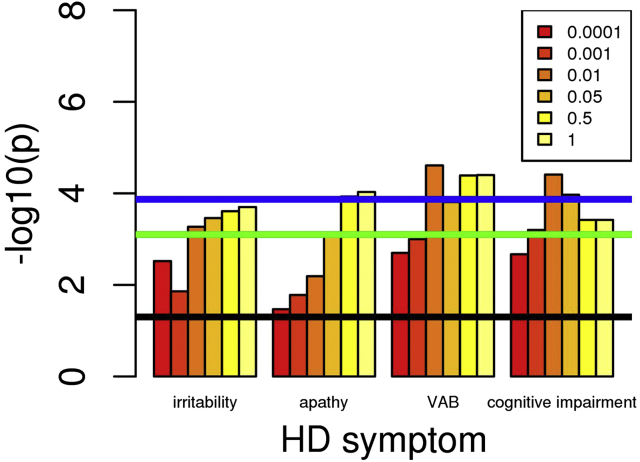
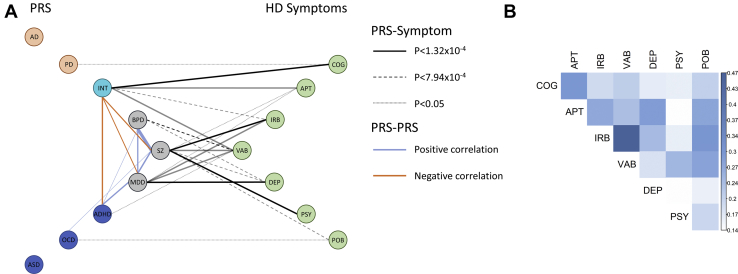
Results: Polygenic risk score for major depression was associated specifically with increased risk of depression in HD, as was schizophrenia risk score with psychosis and irritability. Cognitive impairment and apathy were associated with reduced polygenic risk score for intelligence.
Conclusions: Polygenic risk scores for psychiatric disorders, particularly depression and schizophrenia, are associated with increased risk of the corresponding psychiatric symptoms in HD, suggesting a common genetic liability. However, the genetic liability to cognitive impairment and apathy appears to be distinct from other psychiatric symptoms in HD. No associations were observed between HD symptoms and risk scores for other neurodegenerative disorders. These data provide a rationale for treatments effective in depression and schizophrenia to be used to treat depression and psychotic symptoms in HD.
Keywords: Cognition; Depression; Huntington’s disease; Polygenic risk; Psychiatric; Schizophrenia.
Copyright © 2020 Society of Biological Psychiatry. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Shared Genetic Risk Between Psychiatric and Cognitive Symptoms in Huntington's Disease and in the General Population.Biol Psychiatry. 2020 May 1;87(9):e25-e27. doi: 10.1016/j.biopsych.2020.02.1180. Biol Psychiatry. 2020. PMID: 32299583 No abstract available.
References
-
- Bates G.P., Dorsey R., Gusella J.F., Hayden M.R., Kay C., Leavitt B.R. Huntington disease. Nat Rev Dis Prim. 2015;1:15005. - PubMed
-
- Craufurd D., Snowden J. Neuropsychiatry and neuropsychology. In: Bates G.P., Tabrizi S.J., Jones L., editors. Huntington’s Disease. 4th ed. Oxford University Press; New York: 2014. pp. 36–65.
-
- Holmans P.A., Massey T.H., Jones L. Genetic modifiers of Mendelian disease: Huntington’s disease and the trinucleotide repeat disorders. Hum Mol Genet. 2017;26:R83–R90. - PubMed
-
- Lee J.-M., Correia K., Loupe J., Kim K.-H., Barker D., Hong E.P. Huntington’s disease onset is determined by length of uninterrupted CAG, not encoded polyglutamine, and is modified by DNA maintenance mechanisms. bioRxiv. 2019
