

Variability in chest compression rate calculations during pediatric cardiopulmonary resuscitation
- PMID: 32088254
- PMCID: PMC7296394
- DOI: 10.1016/j.resuscitation.2020.01.040
Variability in chest compression rate calculations during pediatric cardiopulmonary resuscitation
Abstract
Aim: The mathematical method used to calculate chest compression (CC) rate during cardiopulmonary resuscitation varies in the literature and across device manufacturers. The objective of this study was to determine the variability in calculated CC rates by applying four published methods to the same dataset.
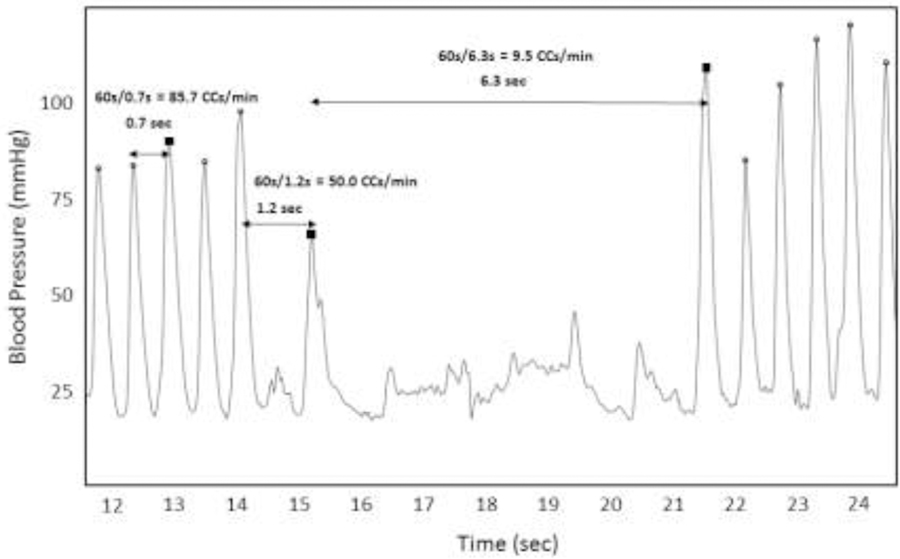
Methods: This study was a secondary investigation of the first 200 pediatric cardiac arrest events with invasive arterial line waveform data in the ICU-RESUScitation Project (NCT02837497). Instantaneous CC rates were calculated during periods of uninterrupted CCs. The defined minimum interruption length affects rate calculation (e.g., if an interruption is defined as a break in CCs ≥ 2 s, the lowest possible calculated rate is 30 CCs/min). Average rates were calculated by four methods: 1) rate with an interruption defined as ≥ 1 s; 2) interruption ≥ 2 s; 3) interruption ≥ 3 s; 4) method #3 excluding top and bottom quartiles of calculated rates. American Heart Association Guideline-compliant rate was defined as 100-120 CCs/min. A clinically important change was defined as ±5 CCs/min. The percentage of events and epochs (30 s periods) that changed Guideline-compliant status was calculated.
Results: Across calculation methods, mean CC rates (118.7-119.5/min) were similar. Comparing all methods, 14 events (7%) and 114 epochs (6%) changed Guideline-compliant status.
Conclusion: Using four published methods for calculating CC rate, average rates were similar, but 7% of events changed Guideline-compliant status. These data suggest that a uniform calculation method (interruption ≥ 1 s) should be adopted to decrease variability in resuscitation science.
Keywords: American Heart Association Guideline; Cardiopulmonary resuscitation; Chest compression rate.
Copyright © 2020 Elsevier B.V. All rights reserved.
Figures
References
-
- Young KD, Seidel JS. Pediatric Cardiopulmonary Resuscitation: A Collective Review. Annals of Emergency Medicine 1999;33(2):195–205. - PubMed
-
- Slonim AD, Patel KM, Ruttimann UE, Pollack MM. Cardiopulmonary Resuscitation in Pediatric Intensive Care Units. Critical Care Medicine 1997;25(12):1951–1955. - PubMed
-
- Girotra S, Nallamothu BK, Spertus JA, et al. Trends in Survival After In-Hospital Cardiac Arrest. Survey of Anesthesiology 2013;57(2): 73–74.
