

A Cross-Sectional Study of Overtreatment and Deintensification of Antidiabetic and Antihypertensive Medications in Diabetes Mellitus: The TEMD Overtreatment Study
- PMID: 32088879
- PMCID: PMC7193034
- DOI: 10.1007/s13300-020-00779-0
A Cross-Sectional Study of Overtreatment and Deintensification of Antidiabetic and Antihypertensive Medications in Diabetes Mellitus: The TEMD Overtreatment Study
Abstract
Introduction: Targeting better glycated hemoglobin (HbA1c) and blood pressure (BP) goals may endanger older adults with type 2 diabetes mellitus (T2DM). Overtreatment of T2DM and hypertension is a trending issue, although undertreatment is still common. We investigated the rates and predictors of overtreatment and undertreatment of glycemia and BP in older adults with T2DM and physicians' attitudes to deintensify or intensify treatment.
Methods: Data from older adults (≥ 65 years) enrolled in a large nationwide T2DM survey in 2017 across Turkey were analyzed. Overtreatment of glycemia was defined as HbA1c < 6.5% plus the use of ≥ 2 oral antihyperglycemics or insulin, and BP overtreatment was defined as systolic BP (SBP) < 120 mmHg or diastolic BP (DBP) < 65 mmHg plus the use of ≥ 2 drugs. Undertreatment of glycemia was defined as HbA1c > 9%, and BP undertreatment was defined as SBP > 150 mmHg or DBP > 90 mmHg. Deintensification or intensification rates were calculated according to treatment modification initiated by the treating physician(s).
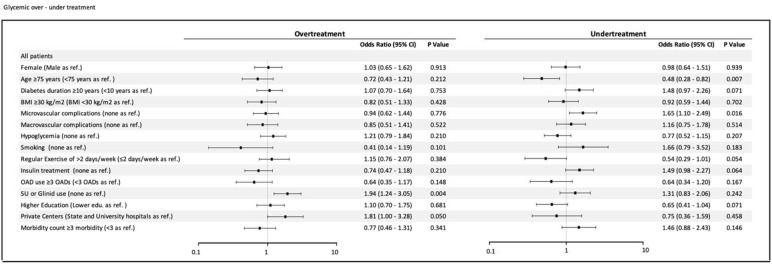
Results: The rate of overtreatment in the glycemia group (n = 1264) was 9.8% (n = 124) and that in the BP group (n = 1052) was 7.3% (n = 77), whereas the rate of undertreatment was 14.2% (n = 180) and 15.2% (n = 160), respectively. In the adjusted model, use of oral secretagogues (sulfonylureas or glinides) (odds ratio [OR] 1.94, 95% confidence interval [CI] 1.2-3.1) and follow-up at a private clinic (OR 1.81, 95% CI 1.0-3.3) were predictors of glycemia overtreatment. BP overtreatment was independently associated with the use insulin-based diabetes therapies (OR 1.86, 95% CI 1.14-3.04). There was no independent association of BP undertreatment to the study confounders. The deintensification and intensification rates were 25 and 75.6%, respectively, for glycemia and 10.9 and 9.2%, respectively, for BP.
Conclusions: The results show that one in ten older adults with T2DM are overtreated while one in four require modification of their current antihyperglycemic and antihypertensive treatments. Physicians are eager to intensify medications while they largely ignore deintensification in diabetes management. These results warrant enforced measures to improve the care of older adults with T2DM.
Trial registration: ClinicalTrials.gov identifier, NCT03455101.
Keywords: Arterial blood pressure; Glycemia; Older adults; Overtreatment; Type 2 diabetes; Undertreatment.
Plain language summary
Type 2 diabetes mellitus (T2DM) is prevalent in the elderly population. Strict glycemia and blood pressure (BP) targets do not improve outcomes but they may increase the rate of adverse events in these patients. Consequently, overtreatment has been an emerging issue in recent years. The overall magnitude of the problem is largely unknown. Therefore, we assessed the rates and predictors of overtreatment and undertreatment of blood glucose and BP in Turkish older adults with T2DM. We also investigated physicians’ reactions to treatment modulation in the overtreated or undertreated patients. Patients participating in the study were: older adults (n = 1264) with T2DM from a cross-sectional, nationwide, multicenter study who followed-up at the same unit during the past 12 months and who did not have decompensated liver disease, psychiatric disorders interfering with cognition or compliance, bariatric surgery in the past 12 months or renal replacement therapy. We found that:
•: • One of ten older adults with T2DM were overtreated for glycemia.
•: • One in four older adults with T2DM required modification of antihyperglycemic treatment with inclusion of the number of insufficiently treated individuals.
•: • One in four older adults with T2DM required modification of antihypertensive treatment.
•: • Physicians are much more inclined to intensify antihyperglycemia medications, while they largely ignore the need for deintensification in the overtreated patients.
•: • Physicians did not modify antihypertensive treatments in about 90% of patients with uncontrolled BP.
•: • Patients who were treated by oral secretagogues and followed in private clinics were most prone to glycemia overtreatment.
•: • Patients who were treated by insulin-based regiments were prone to BP overtreatment.
•: These results suggest that measures should be taken to improve physician awareness of drug modification in older patients with T2DM.
Figures

Comment in
-
HbA1c-Zielkorridor besser beachten! : Diabtetes und Hypertonie.MMW Fortschr Med. 2020 Jun;162(12):28. doi: 10.1007/s15006-020-0605-6. MMW Fortschr Med. 2020. PMID: 32578102 Review. German. No abstract available.
References
-
- Hogan P, Dall T, Nikolov P. Economic costs of diabetes in the US in 2002. Diabetes Care. 2003;26:917–932. - PubMed
-
- Ogurtsova K, da Rocha Fernandes JD, Huang Y, et al. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract. 2017;128:40–50. - PubMed
-
- Selvin E, Coresh J, Brancati FL. The burden and treatment of diabetes in elderly individuals in the US. Diabetes Care. 2006;29:2415–2419. - PubMed
-
- Greenfield S, Billimek J, Pellegrini F, et al. Comorbidity affects the relationship between glycemic control and cardiovascular outcomes in diabetes: a cohort study. Ann Intern Med. 2009;151:854–860. - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
