

Effectiveness of comprehensive cardiac rehabilitation in coronary artery disease patients treated according to contemporary evidence based medicine: Update of the Cardiac Rehabilitation Outcome Study (CROS-II)
- PMID: 32089005
- PMCID: PMC7564293
- DOI: 10.1177/2047487320905719
Effectiveness of comprehensive cardiac rehabilitation in coronary artery disease patients treated according to contemporary evidence based medicine: Update of the Cardiac Rehabilitation Outcome Study (CROS-II)
Abstract
Background: Despite numerous studies and meta-analyses the prognostic effect of cardiac rehabilitation is still under debate. This update of the Cardiac Rehabilitation Outcome Study (CROS II) provides a contemporary and practice focused approach including only cardiac rehabilitation interventions based on published standards and core components to evaluate cardiac rehabilitation delivery and effectiveness in improving patient prognosis.
Design: A systematic review and meta-analysis.
Methods: Randomised controlled trials and retrospective and prospective controlled cohort studies evaluating patients after acute coronary syndrome, coronary artery bypass grafting or mixed populations with coronary artery disease published until September 2018 were included.
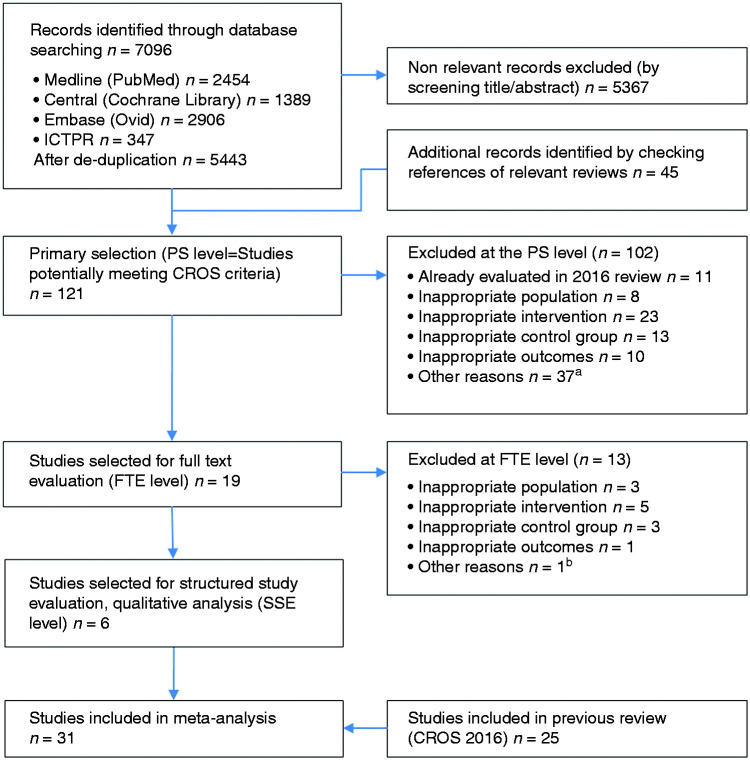
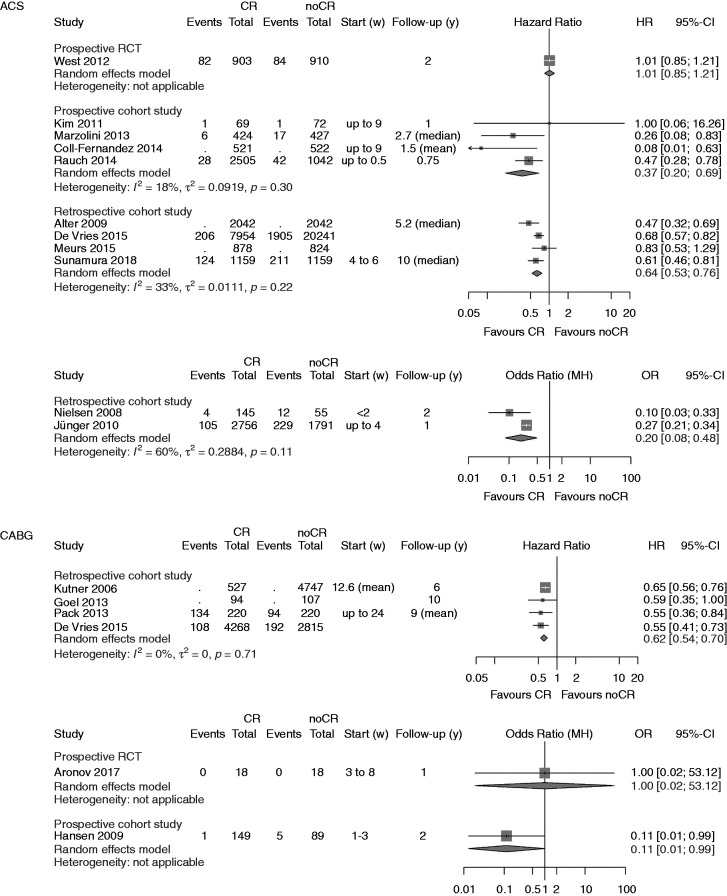
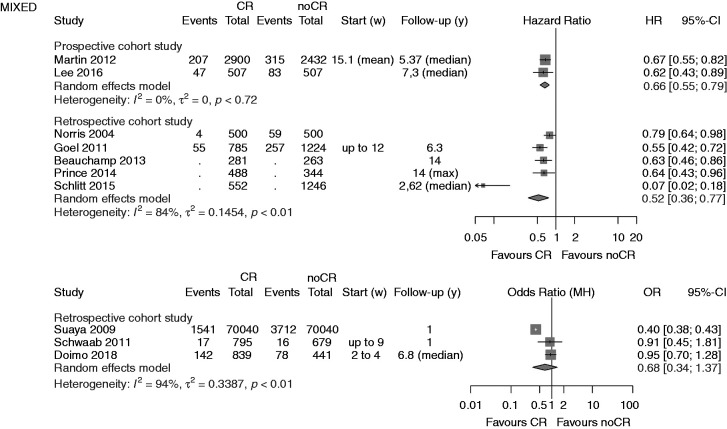
Results: Based on CROS inclusion criteria out of 7096 abstracts six additional studies including 8671 patients were identified (two randomised controlled trials, two retrospective controlled cohort studies, two prospective controlled cohort studies). In total, 31 studies including 228,337 patients were available for this meta-analysis (three randomised controlled trials, nine prospective controlled cohort studies, 19 retrospective controlled cohort studies; 50,653 patients after acute coronary syndrome 14,583, after coronary artery bypass grafting 163,101, mixed coronary artery disease populations; follow-up periods ranging from 9 months to 14 years). Heterogeneity in design, cardiac rehabilitation delivery, biometrical assessment and potential confounders was considerable. Controlled cohort studies showed a significantly reduced total mortality (primary endpoint) after cardiac rehabilitation participation in patients after acute coronary syndrome (prospective controlled cohort studies: hazard ratio (HR) 0.37, 95% confidence interval (CI) 0.20-0.69; retrospective controlled cohort studies HR 0.64, 95% CI 0.53-0.76; prospective controlled cohort studies odds ratio 0.20, 95% CI 0.08-0.48), but the single randomised controlled trial fulfilling the CROS inclusion criteria showed neutral results. Cardiac rehabilitation participation was also associated with reduced total mortality in patients after coronary artery bypass grafting (retrospective controlled cohort studies HR 0.62, 95% CI 0.54-0.70, one single randomised controlled trial without fatal events), and in mixed coronary artery disease populations (retrospective controlled cohort studies HR 0.52, 95% CI 0.36-0.77; two out of 10 controlled cohort studies with neutral results).
Conclusion: CROS II confirms the effectiveness of cardiac rehabilitation participation after acute coronary syndrome and after coronary artery bypass grafting in actual clinical practice by reducing total mortality under the conditions of current evidence-based coronary artery disease treatment. The data of CROS II, however, underscore the urgent need to define internationally accepted minimal standards for cardiac rehabilitation delivery as well as for scientific evaluation.
Keywords: Cardiac rehabilitation; acute coronary syndrome; cardiac rehabilitation delivery; coronary artery disease; coronary bypass grafting; mortality.
Figures
References
-
- Ford ES, Ajani UA, Croft JB, et al. Explaining the decrease in U.S. deaths from coronary disease, 1980–2000. N Engl J Med 2007; 356: 2388–2398. - PubMed
-
- Puymirat E, Simon T, Cayla G, et al. Acute myocardial infarction: changes in patient characteristics, management, and 6-month outcomes over a period of 20 years in the FAST-MI Program (French Registry of Acute ST-Elevation or Non-ST-Elevation Myocardial Infarction) 1995 to 2015. Circulation 2017; 136: 1908–1919. - PubMed
-
- Szummer K, Wallentin L, Lindhagen L, et al. Relations between implementation of new treatments and improved outcomes in patients with non-ST-elevation myocardial infarction during the last 20 years: experiences from SWEDEHEART registry 1995 to 2014. Eur Heart J 2018; 39: 3766–3776. - PubMed
-
- Rauch B, Davos CH, Doherty P, et al. The prognostic effect of cardiac rehabilitation in the era of acute revascularisation and statin therapy: a systematic review and meta-analysis of randomized and non-randomized studies – The Cardiac Rehabilitation Outcome Study (CROS). Eur J Prev Cardiol 2016; 23: 1914–1939. - PMC - PubMed
-
- Piepoli MF, Corra U, Adamopoulos S, et al. Secondary prevention in the clinical management of patients with cardiovascular diseases. Core components, standards and outcome measures for referral and delivery: a policy statement from the cardiac rehabilitation section of the European Association for Cardiovascular Prevention & Rehabilitation. Endorsed by the Committee for Practice Guidelines of the European Society of Cardiology. Eur J Prev Cardiol 2014; 21: 664–681. - PubMed
